2) Well-designed rehabilitation programs for ITB pain aim to progressively overload the injured runner and the ITB to restore tolerance running-specific loads. The loads are not so excessive that the injured ITB is further irritated by extending into tissue overload. 
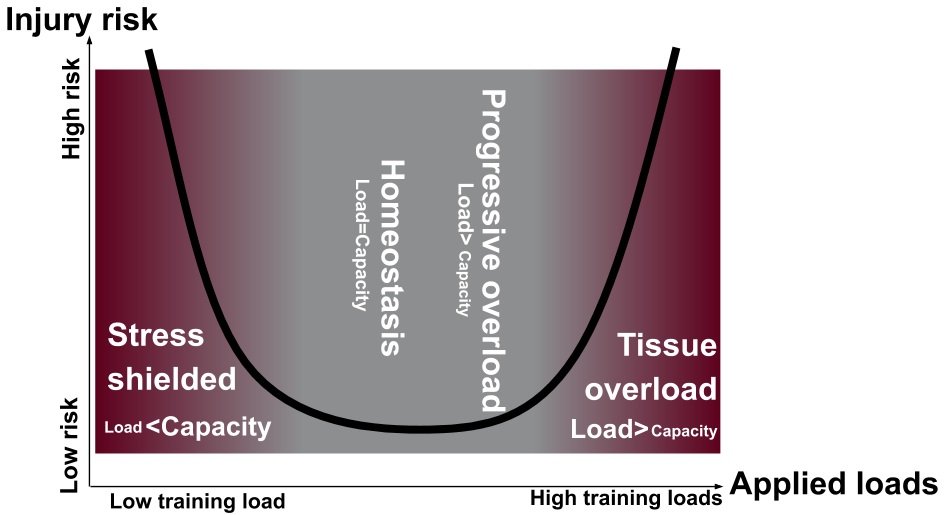
3) Stress shielding, however, is as likely to cause re-injury as tissue overload because the runner will not be adequately prepared for the biomechanical loads that will be encountered during the return-to-run process.

4) Foam rolling is often prescribed for ITB pain. However, foam rolling does not result in changes in flexibility that last more than just a few minutes. ITB pain is likely a compression injury, so it makes little sense to add further compression to the lateral knee.

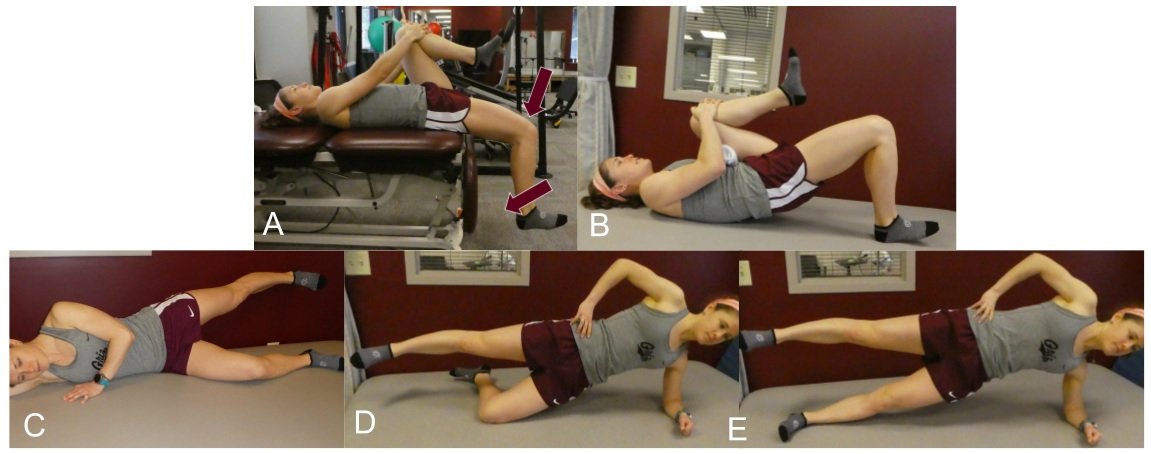
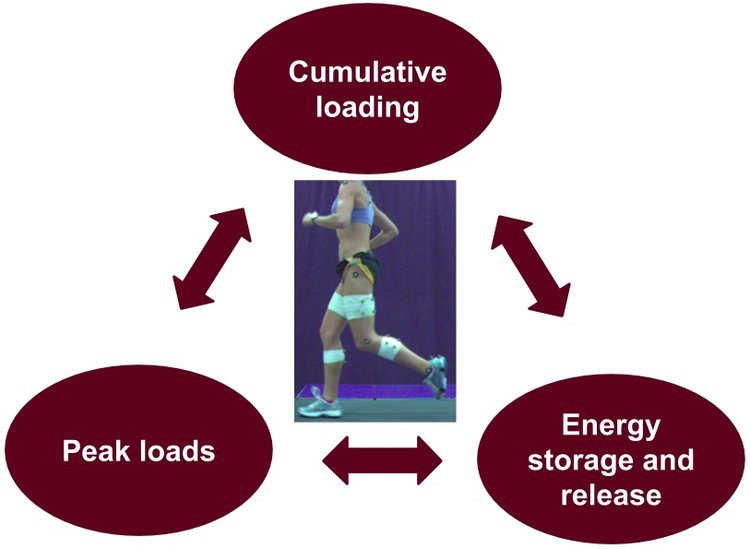
5) During a typical run, anatomical structures experience a) high peak loads; b) with high levels of energy storage and release; c) in a highly cumulative manner. All three of these components of loading should be addressed during rehabilitation.
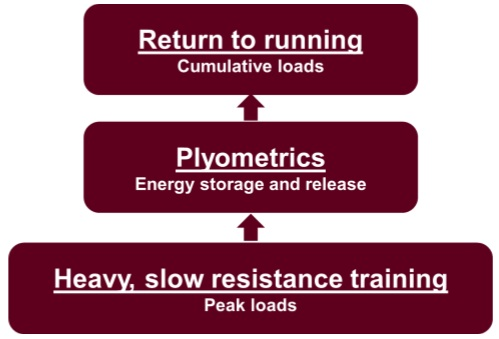
6) Peak loads are addressed with heavy, slow resistance training; energy storage and release demands are addressed with plyometric exercises; and, cumulative loading should be addressed by a graded return-to-run program.
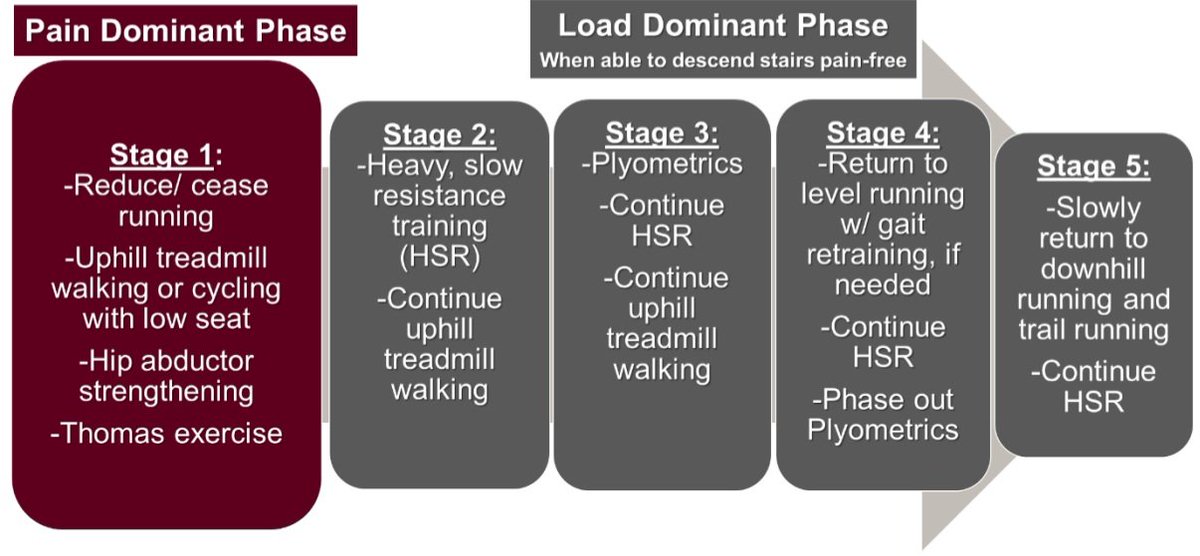
7) ITB pain rehabilitation is divided into two main phases; a) Pain Dominant phase and b) Load Dominant phase (Figure 3). These phases are derived from previous works of @ProfJillCook and Purdam (2009) and Fredericson and Weir (2005).
8) Thanks for making it to the end 🙏🏻
👉🏻 Want to learn more about ITB pain rehab? Read this excellent blog by Rich Willy:
‘Iliotibial Band Pain in the Runner Part 2: Treatment’
physio-network.com/blog/iliotibia…
👉🏻 Want to learn more about ITB pain rehab? Read this excellent blog by Rich Willy:
‘Iliotibial Band Pain in the Runner Part 2: Treatment’
physio-network.com/blog/iliotibia…
• • •
Missing some Tweet in this thread? You can try to
force a refresh