1/16
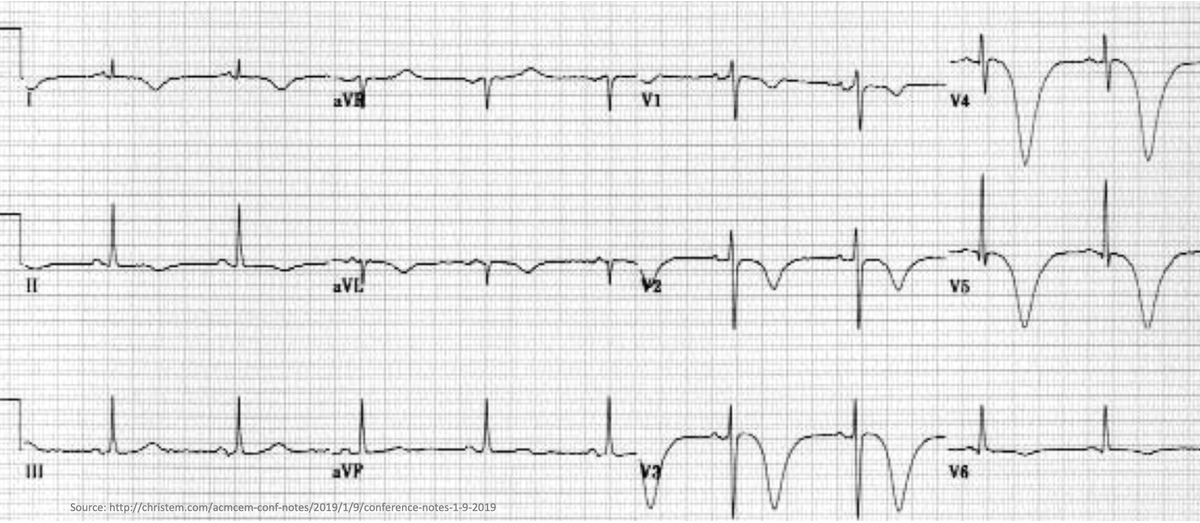
🤔Why does subarachnoid hemorrhage lead to deep/inverted "cerebral T-waves"?
This ECG finding is so dramatic. But as we will see, these patients often have normal hearts.
Why does an issue in the brain manifest on a test of the heart?
🤔Why does subarachnoid hemorrhage lead to deep/inverted "cerebral T-waves"?
This ECG finding is so dramatic. But as we will see, these patients often have normal hearts.
Why does an issue in the brain manifest on a test of the heart?
2/
Cerebral T-waves have been observed for decades.
🔑Though they have been seen in multiple forms of stroke, subarachnoid hemorrhage (SAH) is most closely linked with their appearance.
pubmed.ncbi.nlm.nih.gov/13313536/
Cerebral T-waves have been observed for decades.
🔑Though they have been seen in multiple forms of stroke, subarachnoid hemorrhage (SAH) is most closely linked with their appearance.
pubmed.ncbi.nlm.nih.gov/13313536/
3/
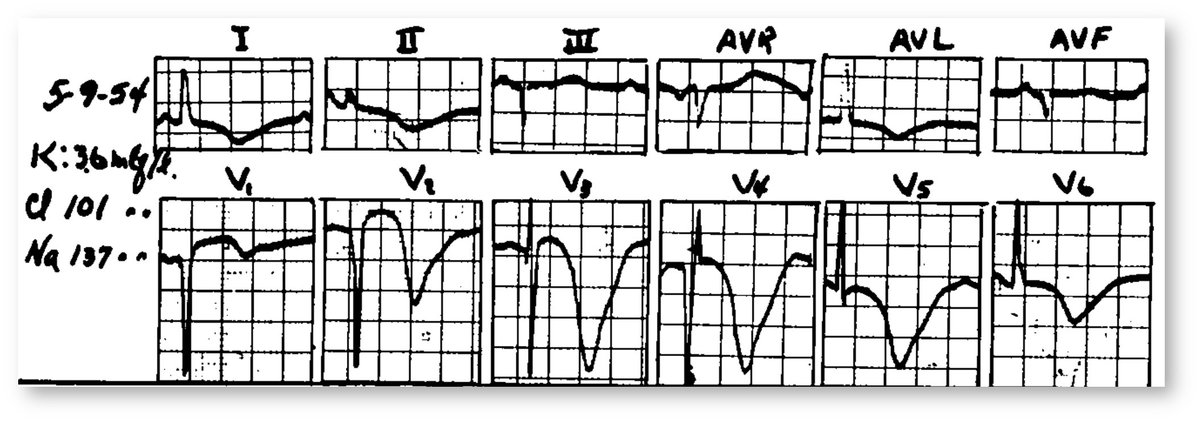
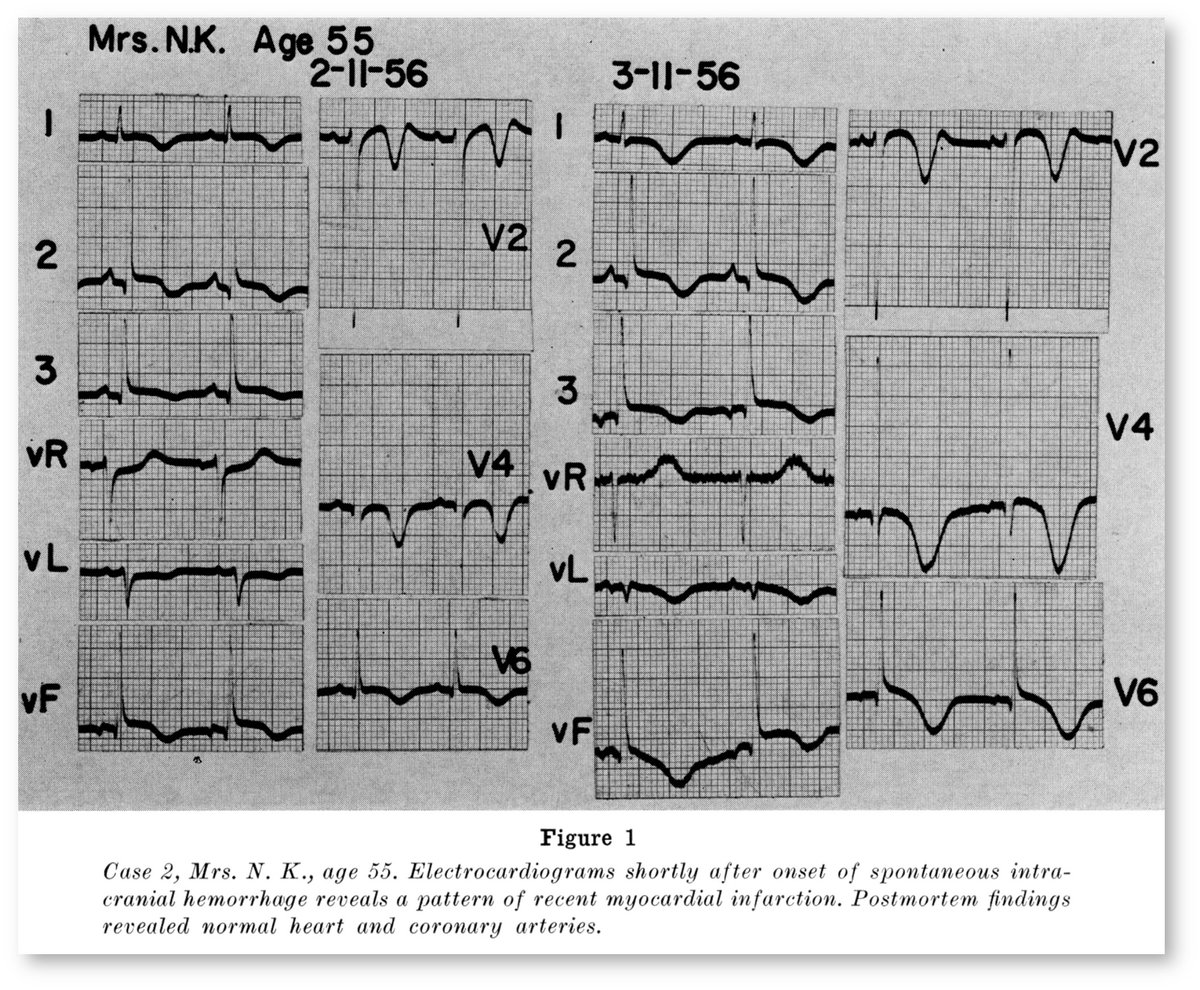
In 1960, Cropp reported a case of T-wave inversions (TWI) secondary to SAH. Surgery was delayed for fear of myocardial infarction (MI).
An autopsy showed no evidence of MI or chronic coronary artery disease.
💡Something else was causing the TWI.
pubmed.ncbi.nlm.nih.gov/13812988/
In 1960, Cropp reported a case of T-wave inversions (TWI) secondary to SAH. Surgery was delayed for fear of myocardial infarction (MI).
An autopsy showed no evidence of MI or chronic coronary artery disease.
💡Something else was causing the TWI.
pubmed.ncbi.nlm.nih.gov/13812988/
4/
Many theories have been proposed to explain cerebral T-waves.
🔑An increase in sympathetic tone, either systemically or localized to the heart, are part of most theories.
pubmed.ncbi.nlm.nih.gov/12138415/
Many theories have been proposed to explain cerebral T-waves.
🔑An increase in sympathetic tone, either systemically or localized to the heart, are part of most theories.
pubmed.ncbi.nlm.nih.gov/12138415/
5/
A 1991 study found that in patients with subarachnoid hemorrhage, high norepinephrine levels were associated with inverted T-waves.
pubmed.ncbi.nlm.nih.gov/2057973/
A 1991 study found that in patients with subarachnoid hemorrhage, high norepinephrine levels were associated with inverted T-waves.
pubmed.ncbi.nlm.nih.gov/2057973/

6/
But not all studies agree. Others have found that plasma norepinephrine concentrations do not parallel electrocardiographic abnormalities.
💡Maybe the sympathetic activity is local, not systemic.
pubmed.ncbi.nlm.nih.gov/8891057/
But not all studies agree. Others have found that plasma norepinephrine concentrations do not parallel electrocardiographic abnormalities.
💡Maybe the sympathetic activity is local, not systemic.
pubmed.ncbi.nlm.nih.gov/8891057/
7/
This possibility was suggested in 1969.
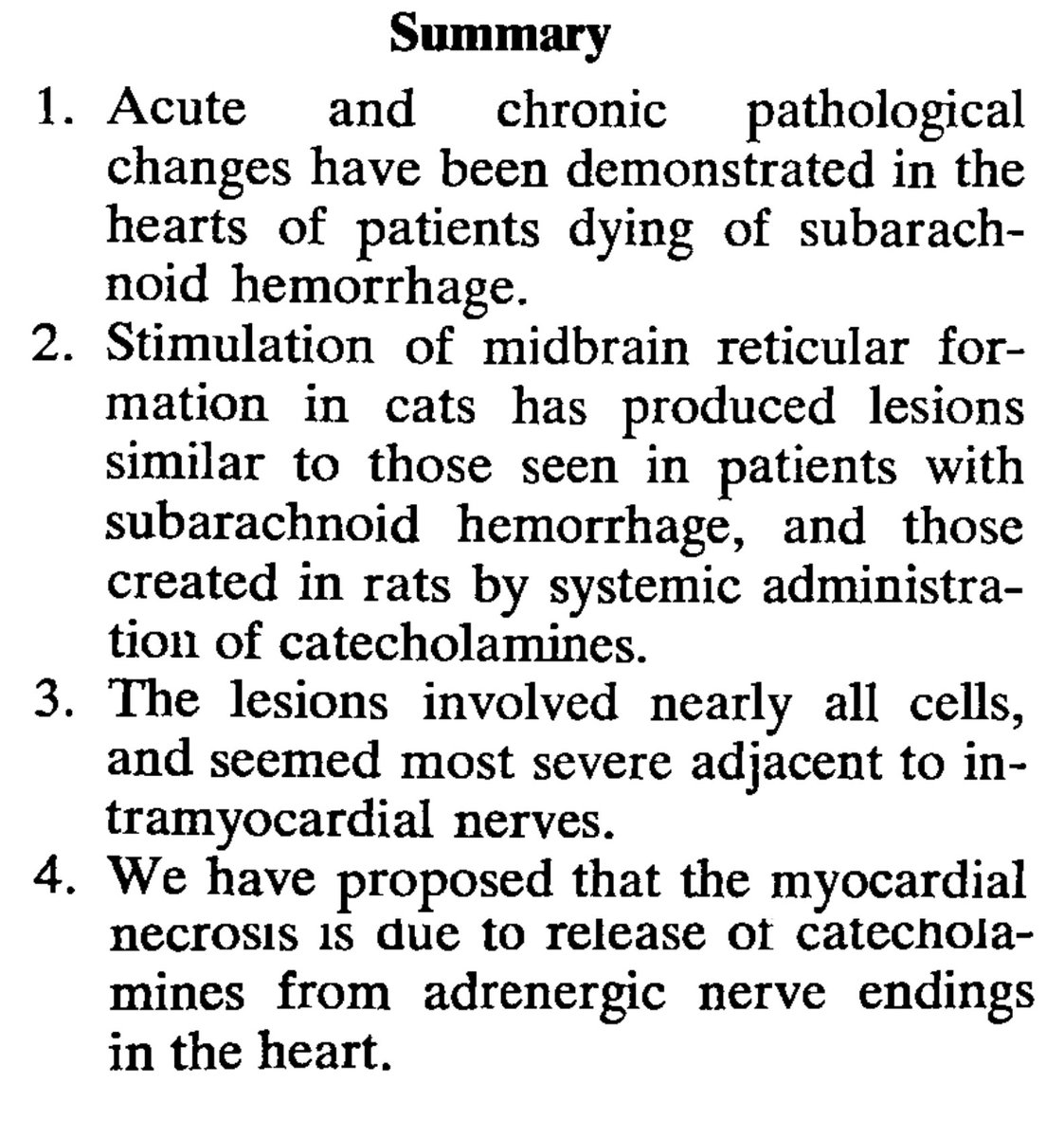
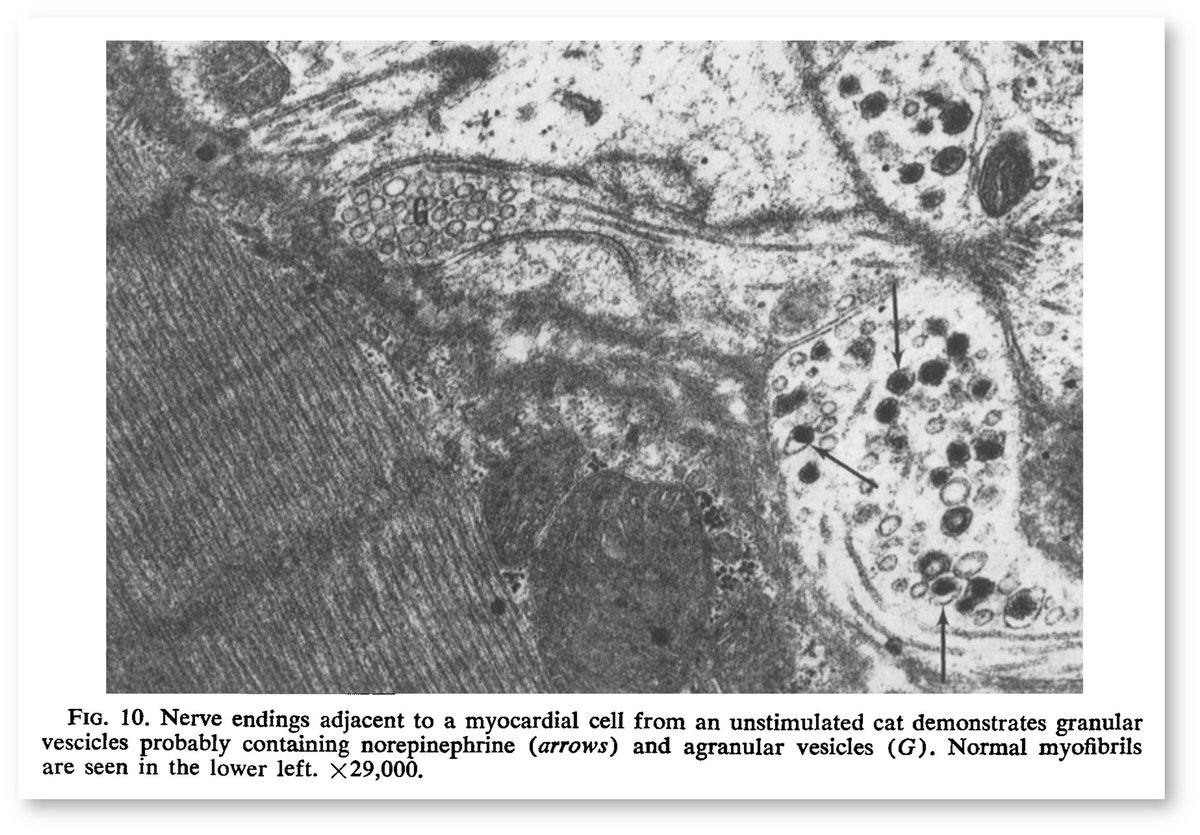
Patients with SAH were found to have myocardial necrosis. But instead of being centered around coronary arteries, it was found near intracardiac nerves!
The damage appeared neural, not ischemic, in origin.
pubmed.ncbi.nlm.nih.gov/5782382/
This possibility was suggested in 1969.
Patients with SAH were found to have myocardial necrosis. But instead of being centered around coronary arteries, it was found near intracardiac nerves!
The damage appeared neural, not ischemic, in origin.
pubmed.ncbi.nlm.nih.gov/5782382/
8/
The results of the study in tweet 7 were felt to be mediated by the LOCAL release of norepinephrine from nerve endings.
🔑Whether systemic or local, sympathetic activation appears to be part of the genesis of cerebral T-waves.
pubmed.ncbi.nlm.nih.gov/5782382/
The results of the study in tweet 7 were felt to be mediated by the LOCAL release of norepinephrine from nerve endings.
🔑Whether systemic or local, sympathetic activation appears to be part of the genesis of cerebral T-waves.
pubmed.ncbi.nlm.nih.gov/5782382/
9/
The question then becomes: how does bleeding into the subarachnoid space lead to sympathetic activation?
To answer this question, we need to examine adjacent structures that might be susceptible to injury after SAH.
The question then becomes: how does bleeding into the subarachnoid space lead to sympathetic activation?
To answer this question, we need to examine adjacent structures that might be susceptible to injury after SAH.
10/
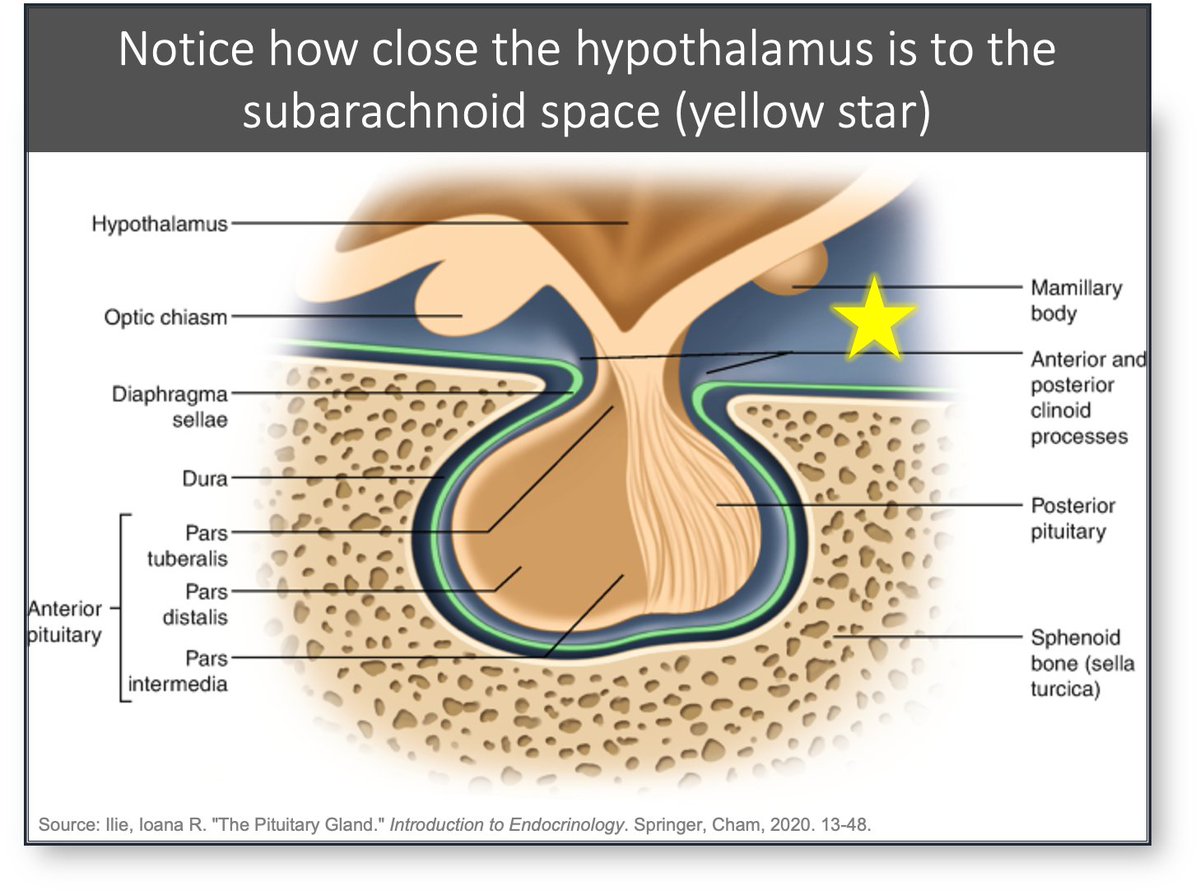
The hypothalamus is one structure adjacent to the subarachnoid space.
Given its role in the autonomic nervous system, one hypothesis suggests that hypothalamic irritation after SAH leads to sympathetic activation and cerebral T-waves.
pubmed.ncbi.nlm.nih.gov/7359184/
The hypothalamus is one structure adjacent to the subarachnoid space.
Given its role in the autonomic nervous system, one hypothesis suggests that hypothalamic irritation after SAH leads to sympathetic activation and cerebral T-waves.
pubmed.ncbi.nlm.nih.gov/7359184/
11/
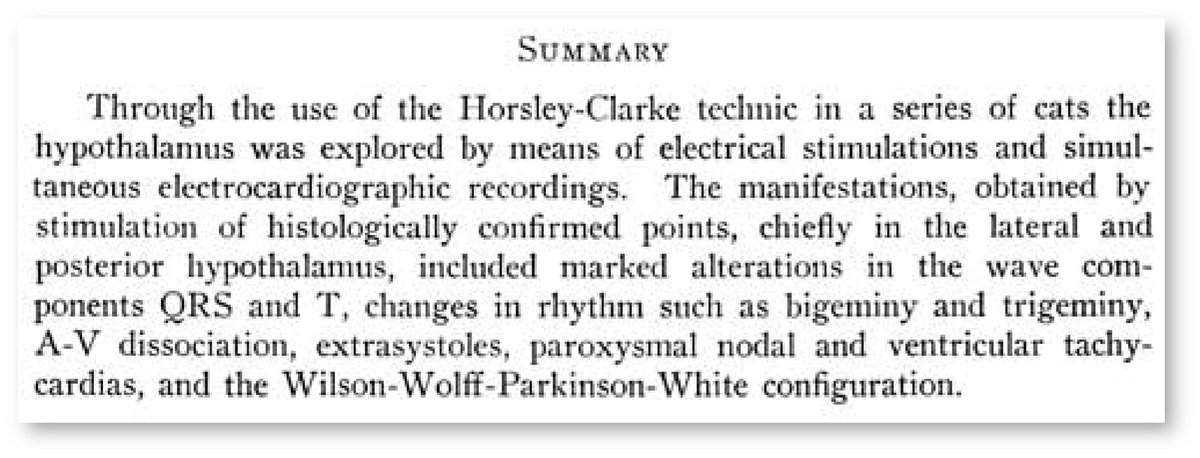
This is supported by animal studies from the 1960s showing that direct electrical stimulation of the hypothalamus leads to ECG changes (including TWI).
pubmed.ncbi.nlm.nih.gov/13843556/
This is supported by animal studies from the 1960s showing that direct electrical stimulation of the hypothalamus leads to ECG changes (including TWI).
pubmed.ncbi.nlm.nih.gov/13843556/
12/
Another structure that may be affected by SAH is the insular cortex, an area that lies buried in the sylvian fissure beneath the frontoparietal and temporal lobes.
🔑The insular cortex also plays a role in sympathetic regulation.
ncbi.nlm.nih.gov/pmc/articles/P…
Another structure that may be affected by SAH is the insular cortex, an area that lies buried in the sylvian fissure beneath the frontoparietal and temporal lobes.
🔑The insular cortex also plays a role in sympathetic regulation.
ncbi.nlm.nih.gov/pmc/articles/P…
13/
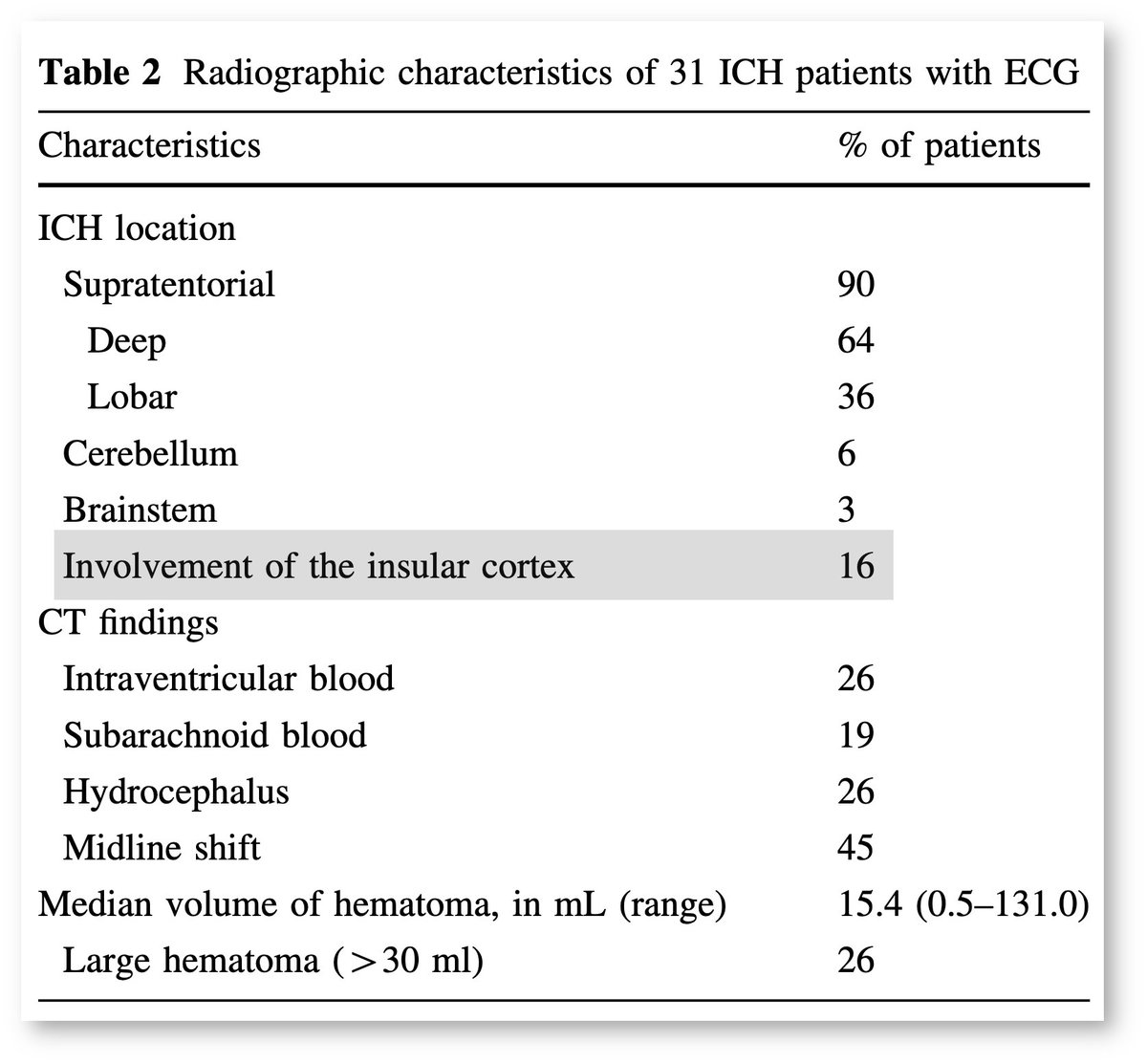
Just as with the hypothalamus, the insular cortex is susceptible to injury after SAH.
💡It may be that damage to the insular cortex leads to sympathetic activation resulting in cerebral T-waves.
pubmed.ncbi.nlm.nih.gov/19813104/
Just as with the hypothalamus, the insular cortex is susceptible to injury after SAH.
💡It may be that damage to the insular cortex leads to sympathetic activation resulting in cerebral T-waves.
pubmed.ncbi.nlm.nih.gov/19813104/
14/
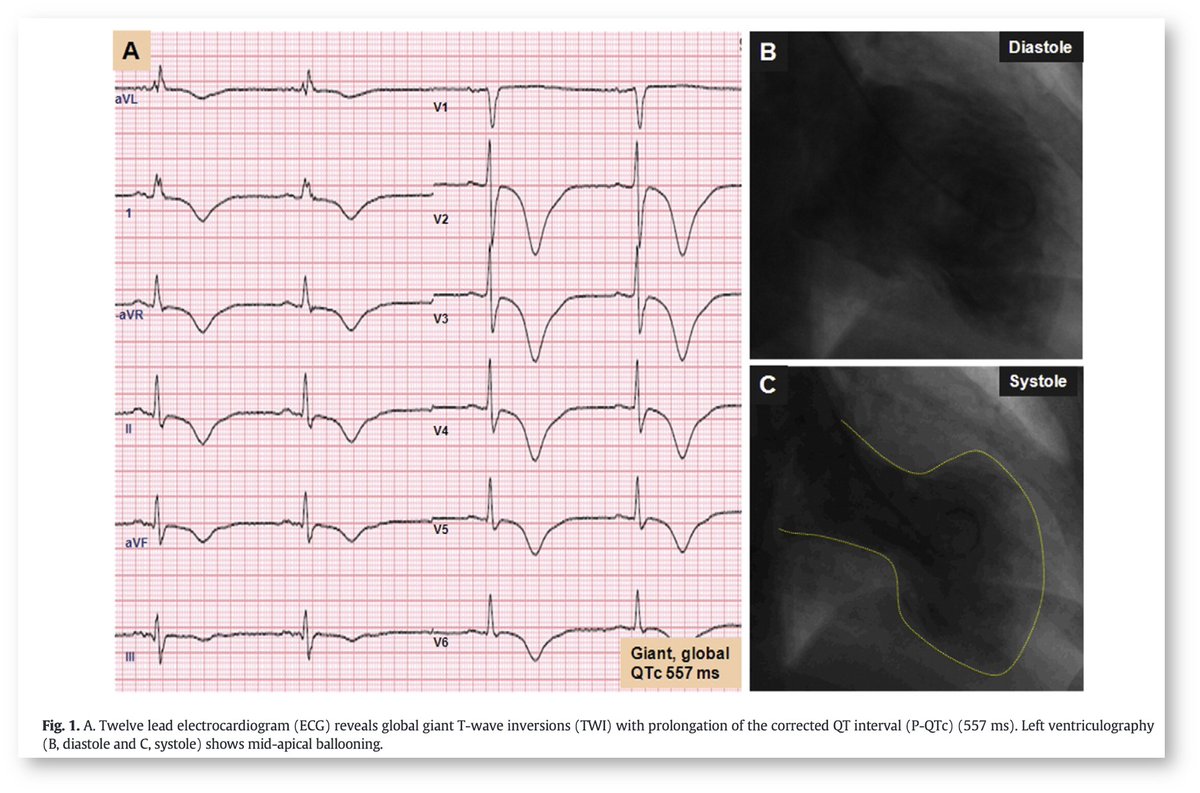
Additional support for the sympathetic activation hypothesis comes from another condition associated with elevated catecholamines and deep/inverted T-waves:
⚡️Takotsubo (stress) cardiomyopathy⚡️
The TWIs are often identical in appearance.
pubmed.ncbi.nlm.nih.gov/25981361/
Additional support for the sympathetic activation hypothesis comes from another condition associated with elevated catecholamines and deep/inverted T-waves:
⚡️Takotsubo (stress) cardiomyopathy⚡️
The TWIs are often identical in appearance.
pubmed.ncbi.nlm.nih.gov/25981361/
15/
Cerebral T-waves in subarachnoid hemorrhage are just one example where sympathetic activation leads to deep TWI.
In the coming days, I'll add some other examples of what might be more accurately termed "sympathetic T-waves".
Cerebral T-waves in subarachnoid hemorrhage are just one example where sympathetic activation leads to deep TWI.
In the coming days, I'll add some other examples of what might be more accurately termed "sympathetic T-waves".
16/16
☞ Subarachnoid hemorrhage is associated with deep/inverted "cerebral T-waves"
☞ Cerebral T-waves are the result of sympathetic activation, either from injury to the hypothalamus and/or insular cortex
☞ Subarachnoid hemorrhage is associated with deep/inverted "cerebral T-waves"
☞ Cerebral T-waves are the result of sympathetic activation, either from injury to the hypothalamus and/or insular cortex
• • •
Missing some Tweet in this thread? You can try to
force a refresh