
1) I'm no expert but the Dolo 650 controversy is either a meaningless or a malignant one.
PCM is an OTC drug --> it is almost never the only drug in a prescription.
Why?
PCM is an OTC drug --> it is almost never the only drug in a prescription.
Why?
2) PCM doesn't provide any significant analgesia unless you are taking 2-3 gm/day.
Its good for the myalgia and arthralgia of febrile illnesses especially if NSAIDs are contraindicated --> like dengue which has a risk of thrombocytopenia.
Its good for the myalgia and arthralgia of febrile illnesses especially if NSAIDs are contraindicated --> like dengue which has a risk of thrombocytopenia.
3) For everything beyond this, you will need an adequate dose of an NSAID +/- local or systemic glucocorticoid therapy --> even DMARDs if its rheumatological!
Most patients in India don't go to a doctor for mild aches and pains --> they will buy PCM directly!
Most patients in India don't go to a doctor for mild aches and pains --> they will buy PCM directly!
4) No doctor will prescribe less than adequate analgesia for a patient in pain --> it is simply unthinkable.
So isolated PCM prescriptions are about as rare as the people who are willing to look beyond cheap media publicity --> it is for their benefit that I have posted this.
So isolated PCM prescriptions are about as rare as the people who are willing to look beyond cheap media publicity --> it is for their benefit that I have posted this.
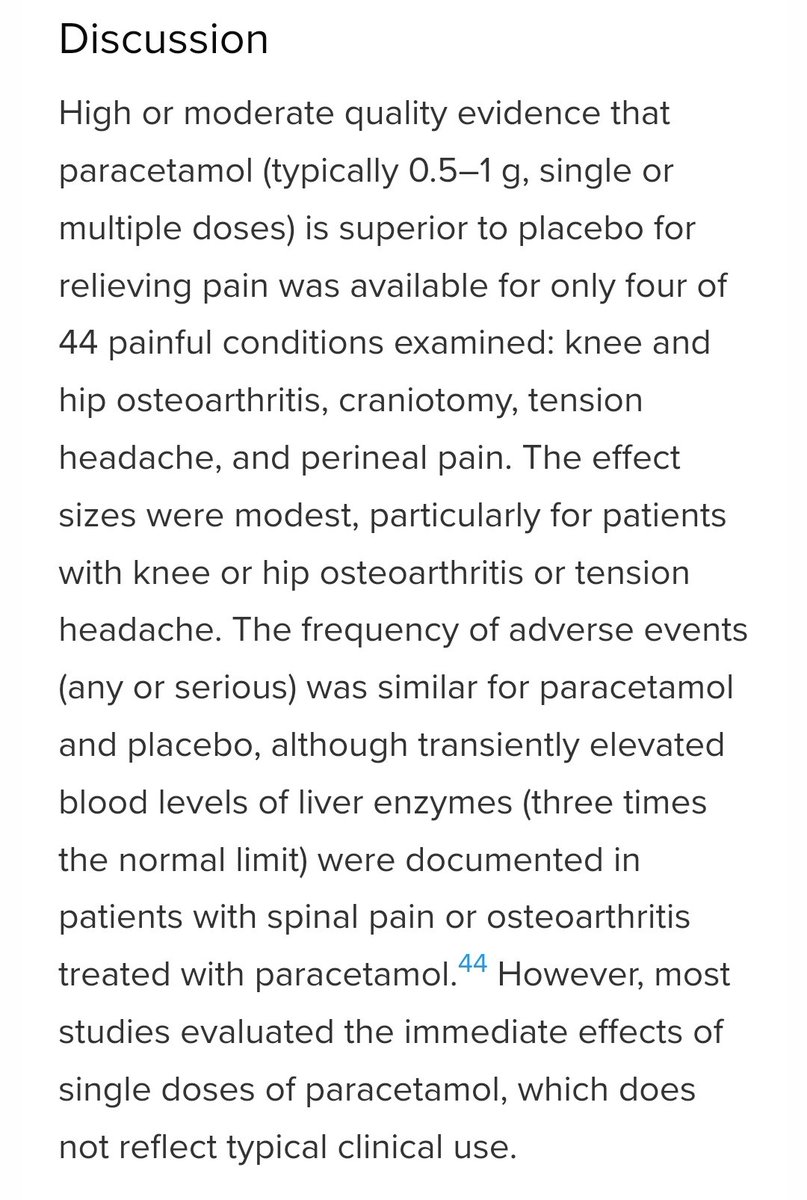
5) This review --> high quality evidence of analgesia is lacking for PCM.
Even then it required a minimum of 1 gm/day and provided only mild analgesia.
PS. It DID NOT WORK in acute low back pain. mja.com.au/journal/2021/2…
Even then it required a minimum of 1 gm/day and provided only mild analgesia.
PS. It DID NOT WORK in acute low back pain. mja.com.au/journal/2021/2…
6) Excerpts from the above article --> adequate analgesia with PCM is impossible because at such high doses --> transient elevation of liver enzymes --> can easily lead to ALF in unmonitored patients. 

7) PCM is safe and well tolerated drug --> especially when used in doses as seen in usual clinical practice --> it also lacks most of the adverse effects of NSAID unless its taken long term.
Its an adjunct.
All physicians use it --> but none rely on it only!
Its an adjunct.
All physicians use it --> but none rely on it only!
8) It is frankly illogical --> if one thinks that docs are dying to prescribe an off patent OTC painkiller with only modest efficacy --> that seasoned pharma executives will pay crores for something like this.
The foolishness, even if its is a conspiracy, boggles the mind!
The foolishness, even if its is a conspiracy, boggles the mind!
*a
• • •
Missing some Tweet in this thread? You can try to
force a refresh


