
Getting my #flozin fix on a Sunday catching up on #ESC2022 #ESCCongress2022 some thoughts in a thread 🧵 @UKCPACardiac @UKCPA @UKCPADiabetes
@escardio @hFRenDsUK
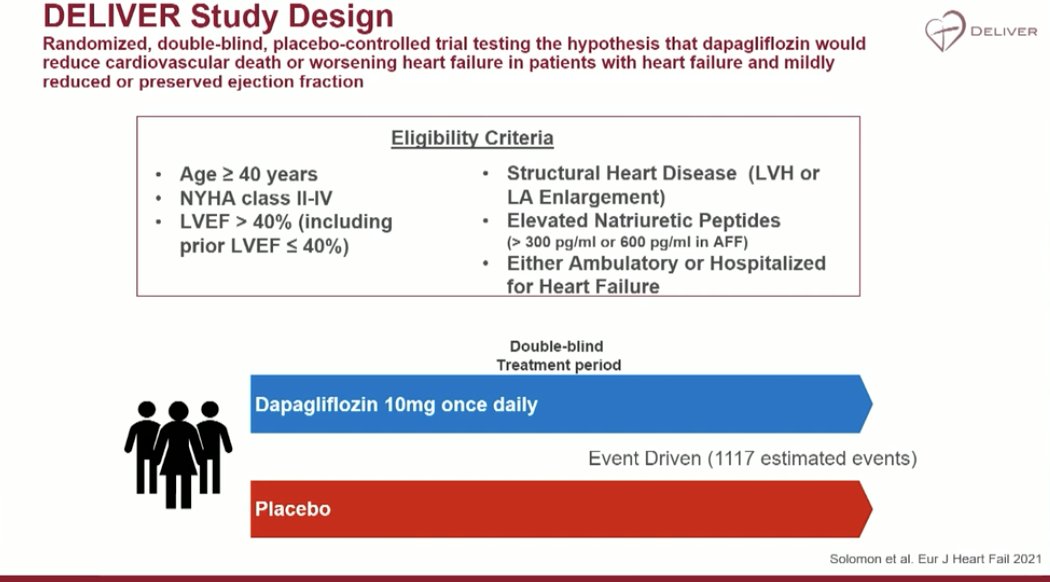
Let's start with the headline, drum roll please 🥁... Dapagliflozin in HFmrEF and HFpEF DELIVER Trial results
@escardio @hFRenDsUK
Let's start with the headline, drum roll please 🥁... Dapagliflozin in HFmrEF and HFpEF DELIVER Trial results
1. Background💔
HFpEF pts represent approx 50% of all people with HF
Currently limited Tx options in this group
Uncertainty remains re:
- People in highest part of EF range, ?attenuation of Tx effect
- People initiated on Tx during/soon after hospitalisation
- EF improved to >40%
HFpEF pts represent approx 50% of all people with HF
Currently limited Tx options in this group
Uncertainty remains re:
- People in highest part of EF range, ?attenuation of Tx effect
- People initiated on Tx during/soon after hospitalisation
- EF improved to >40%
2. Trial design, Endpoints and Flow
Note: either ambulatory or hospitalised patients
6236 patients. 3131 received dapagliflozin. Across 20 countries 🗺️
Follow up - 2.3 years
Equal drop out and incomplete follow up in Tx and in placebo arms
Note: either ambulatory or hospitalised patients
6236 patients. 3131 received dapagliflozin. Across 20 countries 🗺️
Follow up - 2.3 years
Equal drop out and incomplete follow up in Tx and in placebo arms


3. Baseline Characteristics
- Including medication 💊 (highest % of pts on MRAs of any trial in HF with mildly reduced and preserved EF at 43%) (77% on loop diuretics)
- 44% of patients with T2DM
- Including medication 💊 (highest % of pts on MRAs of any trial in HF with mildly reduced and preserved EF at 43%) (77% on loop diuretics)
- 44% of patients with T2DM


4. Primary Endpoint - CV death, worsening HF
NNT of 32
Very little difference between full population and population with LVEF < 60%
Worsening HF reduced⬇️by 21%
CV death reduced ⬇️by 12% (non-significant)
Overall reduced primary endpoint by 18%
NNT of 32
Very little difference between full population and population with LVEF < 60%
Worsening HF reduced⬇️by 21%
CV death reduced ⬇️by 12% (non-significant)
Overall reduced primary endpoint by 18%



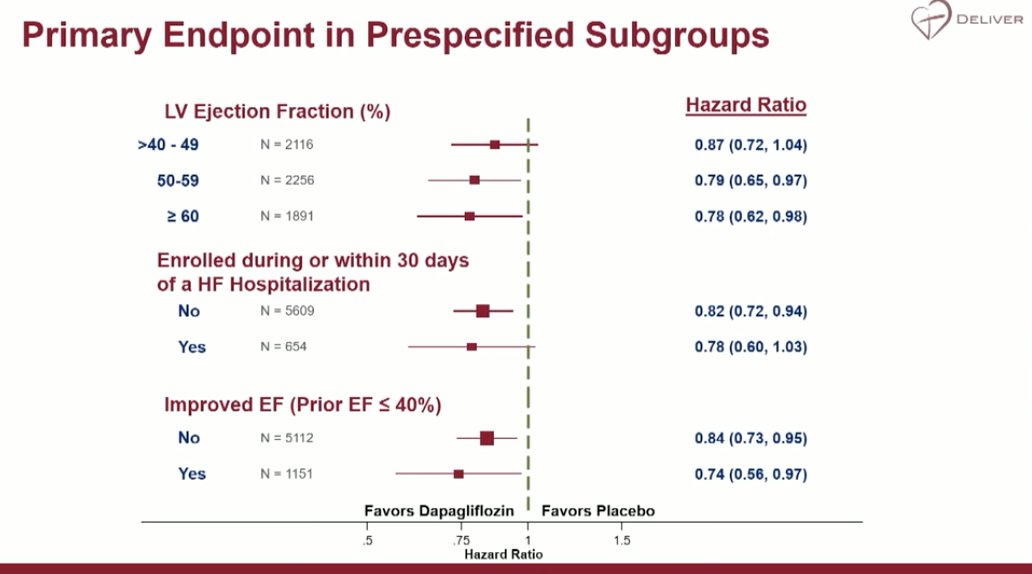
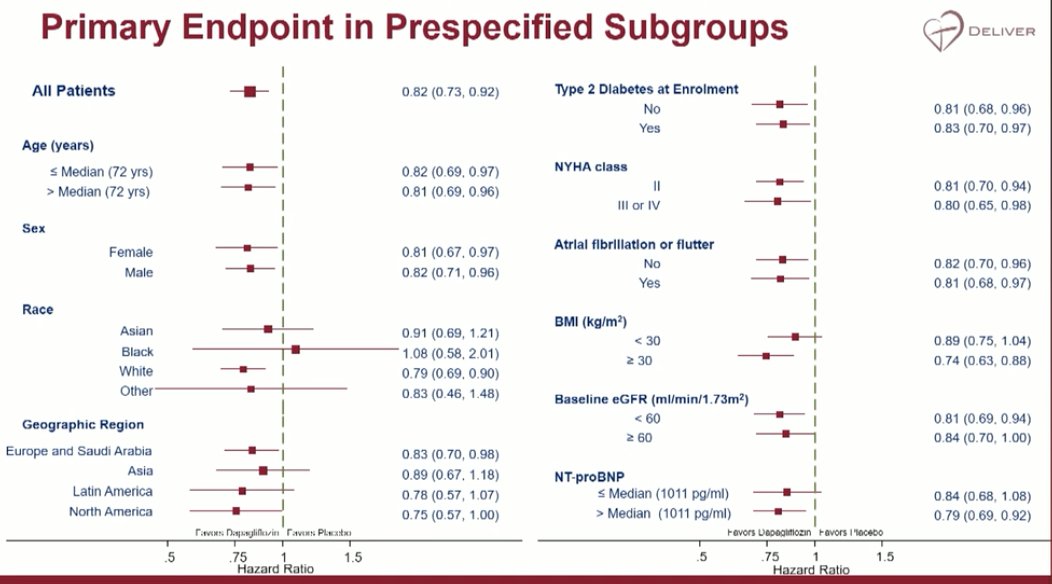
5. Further endpoint results
- no evidence of attenuation in higher EF group
- similar benefit seen in pts enrolled during or within 30 days of HF hospitalisation compared
Very consistent across subgroups/characteristics
- no evidence of attenuation in higher EF group
- similar benefit seen in pts enrolled during or within 30 days of HF hospitalisation compared
Very consistent across subgroups/characteristics
6. Adverse Events
- 2 incidents of DKA
- 6 major hypoglycaemic events (NB: less than placebo)
- 19 amputations (NB: less than placebo)
- 2 incidents of DKA
- 6 major hypoglycaemic events (NB: less than placebo)
- 19 amputations (NB: less than placebo)

7. Safe to say I think that DELIVER has DELIVERED. 🚚📮
But what about Empagliflozin in EMPEROR-Preserved I hear you cry...
But what about Empagliflozin in EMPEROR-Preserved I hear you cry...
8. Comparable primary endpoints, principle effects and similar populations used
New information from DELIVER:
- Efficacy in those with improved/recovered LVEF
- Benefit across LVEF categories
EMPEROR-Preserved suggested some attenuation of effects of empa at higher EF
New information from DELIVER:
- Efficacy in those with improved/recovered LVEF
- Benefit across LVEF categories
EMPEROR-Preserved suggested some attenuation of effects of empa at higher EF


9. Want to read more - lovely meta-analysis paper here: thelancet.com/journals/lance…
10. How this may change our day to day practice...
Is it time to move away from EF? HF is not a single pathological diagnosis, or a single disease, it is hundreds of diseases, it is a syndrome. How do we move to a more personalised Tx approach?
Is it time to move away from EF? HF is not a single pathological diagnosis, or a single disease, it is hundreds of diseases, it is a syndrome. How do we move to a more personalised Tx approach?


11. But the question still remains.. how do SGLT2 inhibitors work in HF - jury still out!
Do we need to understand this more to advance even further... @DrRaniKhatib @PharmacistHF @HAM2A_K @JanineBeezer @PharmRJ @Ines_VFonseca @GoggleDocs
Do we need to understand this more to advance even further... @DrRaniKhatib @PharmacistHF @HAM2A_K @JanineBeezer @PharmRJ @Ines_VFonseca @GoggleDocs

• • •
Missing some Tweet in this thread? You can try to
force a refresh










