A 🧵for anyone prescribing, monitoring or seeing people on drug Tx for HF from @escardio #esc2022
"The practicalities of drug treatment in HF" 💔💊 with lots and lots of top tips⤵️
Great advice from conference that you can apply day to day! @GoggleDocs @UKCPACardiac @UKCPA
"The practicalities of drug treatment in HF" 💔💊 with lots and lots of top tips⤵️
Great advice from conference that you can apply day to day! @GoggleDocs @UKCPACardiac @UKCPA
ESC Guidelines for HFrEF treatment:
Look at the quality of that evidence and recommendations for drug Tx! 😃💊
Look at the quality of that evidence and recommendations for drug Tx! 😃💊

Beta-blockers:
- start low, go slow
- ALWAYS titrate 📈for maximum benefit
- intolerance likely to resolve with time ⏲️
- start low, go slow
- ALWAYS titrate 📈for maximum benefit
- intolerance likely to resolve with time ⏲️


MRAs:
- minimal impact on BP
- watch that K! (Include dietary advice 🥗)
- minimal impact on BP
- watch that K! (Include dietary advice 🥗)

ARNI (Sacubitril/Valsartan):
- Going direct to ARNI is well tolerated
- STOP🛑ACEi 36 hours to reduce risk of angioedema
- Lowest dose drops BP the most, so there is more scope for titration than you may think 💊📈
- Going direct to ARNI is well tolerated
- STOP🛑ACEi 36 hours to reduce risk of angioedema
- Lowest dose drops BP the most, so there is more scope for titration than you may think 💊📈


SGLT2 inhibitors:
- Quick benefit (2-4 weeks)
- How do they work in HF?!?! (Let's be honest we still don't really know!🤔 But we do know they work!)
- Ideal across any clinical presentation of HF
- Watch out for adverse effects
- Renal function will drop - don't STOP the SGLT2
- Quick benefit (2-4 weeks)
- How do they work in HF?!?! (Let's be honest we still don't really know!🤔 But we do know they work!)
- Ideal across any clinical presentation of HF
- Watch out for adverse effects
- Renal function will drop - don't STOP the SGLT2


So which drug when?? 💊⏲️
Current problem, not practical, too slow
Current problem, not practical, too slow

Old vs new ESC Guidelines:
Starting to think about horizontal initiation. Currently lacking evidence in this area.
Starting to think about horizontal initiation. Currently lacking evidence in this area.

How do we speed up titration and what is the best order of drug initiation in HF?
From trial modelling these regimens came out top:
Note different order to reduce CV death vs reducing CV death and HF hospitalisation
From trial modelling these regimens came out top:
Note different order to reduce CV death vs reducing CV death and HF hospitalisation


Is this the future of HF treatment pathways? 🤔

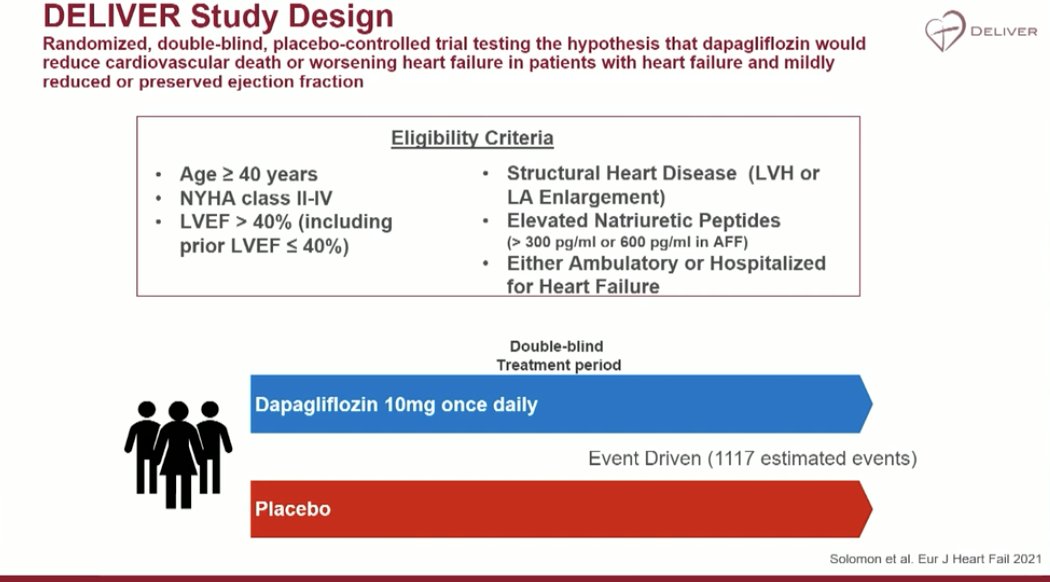
Hospitalisation is an opportunity to give HFrEF drugs. EMPULSE and SOLOIST and now DELIVER showed safety in hospitalised patients
Don't forget individual patients need individualised pathways. One size won't fit all. Trials are needed in this area to determine best sequence
Don't forget individual patients need individualised pathways. One size won't fit all. Trials are needed in this area to determine best sequence




Last but not least, HFpEF and HFmrEF:


ESC recommend 'concomitant implementation' of the four pillars
⬆️💊Uptitration should be according to pt phenotype rather than target doses
⬆️💊Uptitration should be according to pt phenotype rather than target doses

• • •
Missing some Tweet in this thread? You can try to
force a refresh