Dr. Koichi Goto starts the lung mini oral session with results from DESTINY-Lung02 of the recently approved trastuzumab deruxtecan in #HER2 NSCLC #ESMO22 

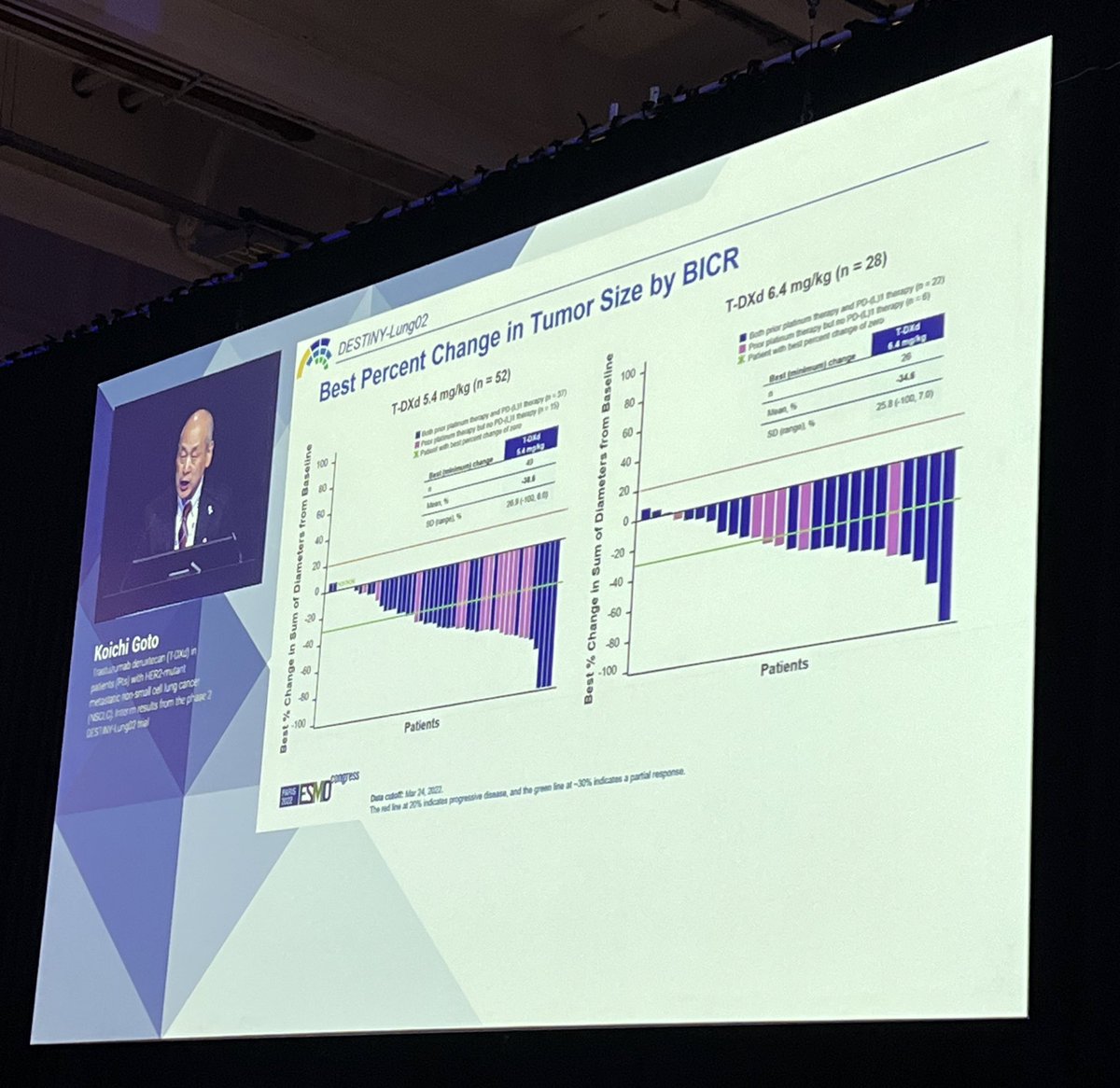
DESTINY-Lung02 compared two doses of trastuzumab deruxtecan (T-DXd) in #HER2 previously treated NSCLC (5.4 mg/kg vs 6.4 mg/kg): RR 58% and DoR 8.7m at the lower dose compared to 43% at 6.4 mg/kg. #ESMO22
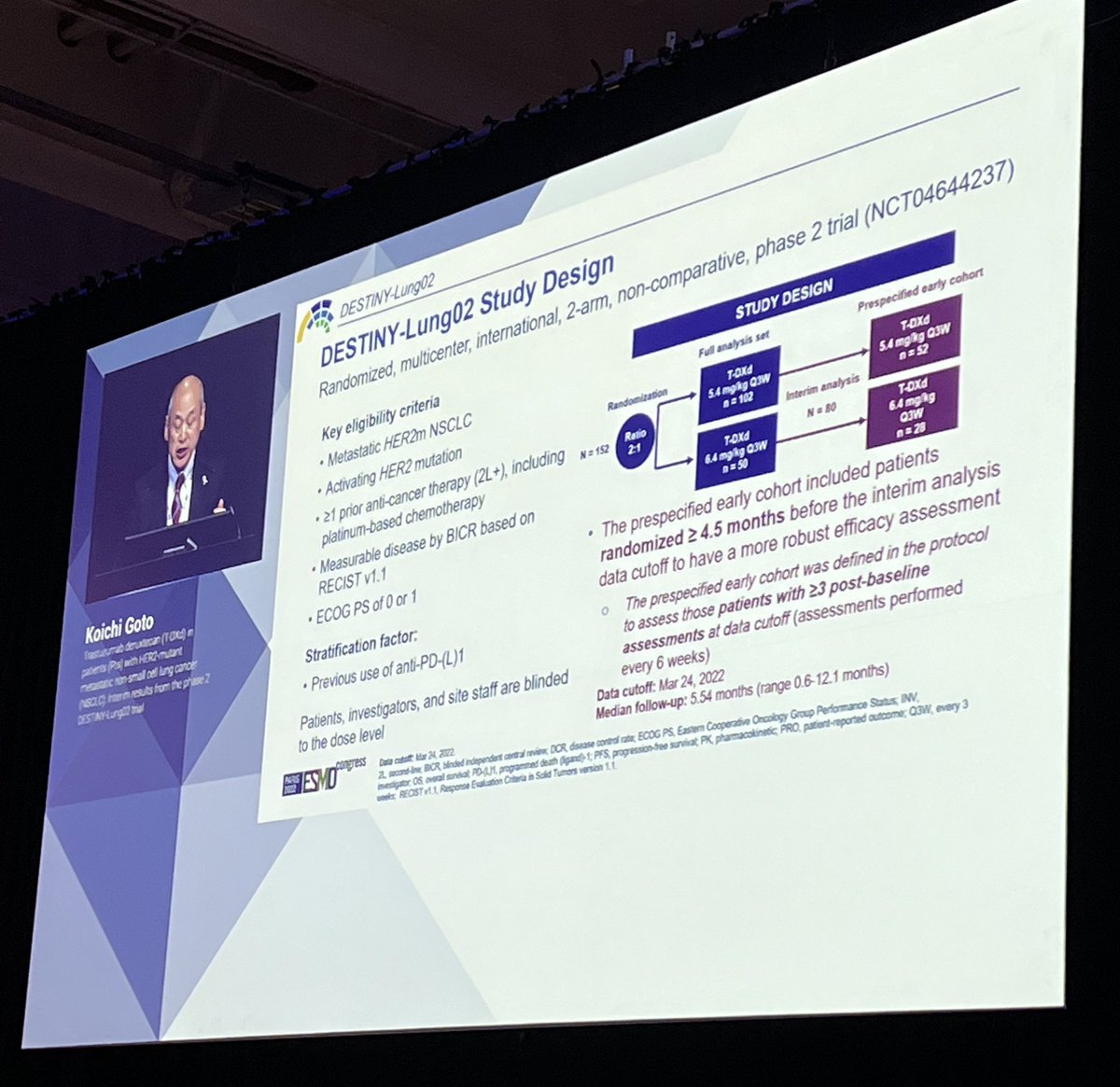


Importantly- interstitial lung disease much less frequent at the 5.4 mg/kg dose (5.9%, only 1 case of G3). This is the FDA approved dose of trastuzumab deruxtecan in #HER2 NSCLC #ESMO22



For a primer on ADCs (antibody drug conjugates) in NSCLC, listen to this episode of the @IASLC podcast, Lung Cancer Considered, where Drs. @benlevylungdoc and @BeccaHeistMD discuss this new (to NSCLC) class of agents. #ESMO22 #LCSM
iaslc.org/iaslc-news/lun…
iaslc.org/iaslc-news/lun…
• • •
Missing some Tweet in this thread? You can try to
force a refresh