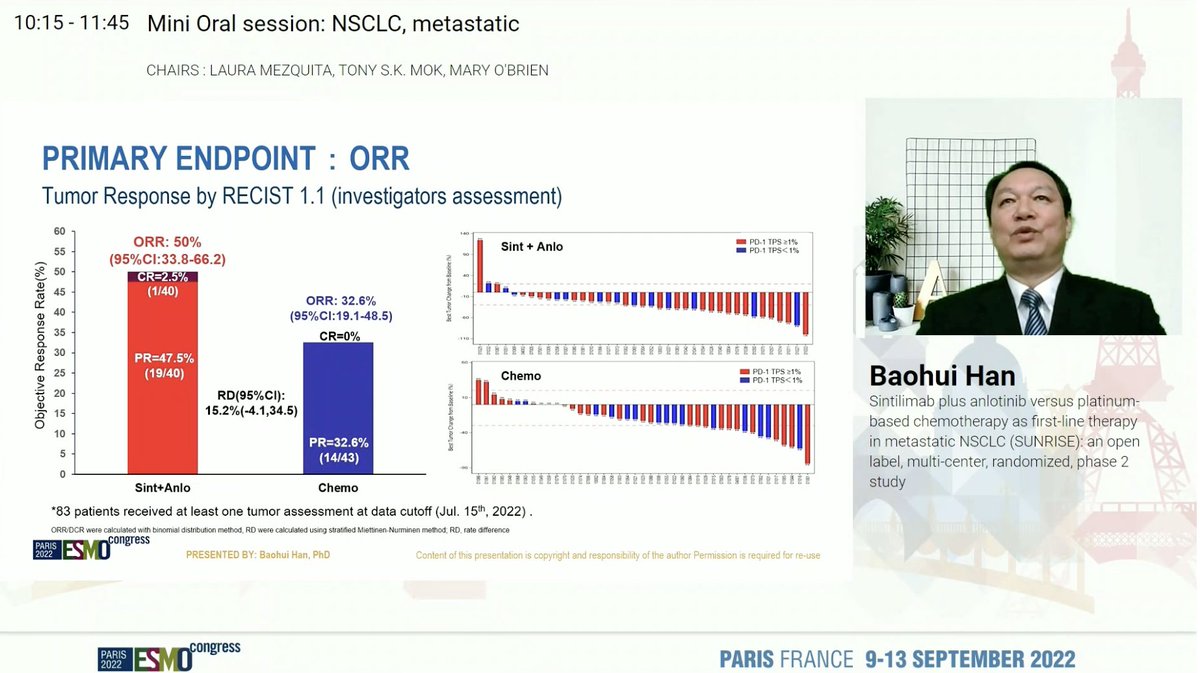
Dr. Baohui Han presents SUNRISE: randomized phase II study of sintilimab (PD1) and anlotinib (anti-angiogenic TKI) in metastatic NSCLC. #ESMO22 

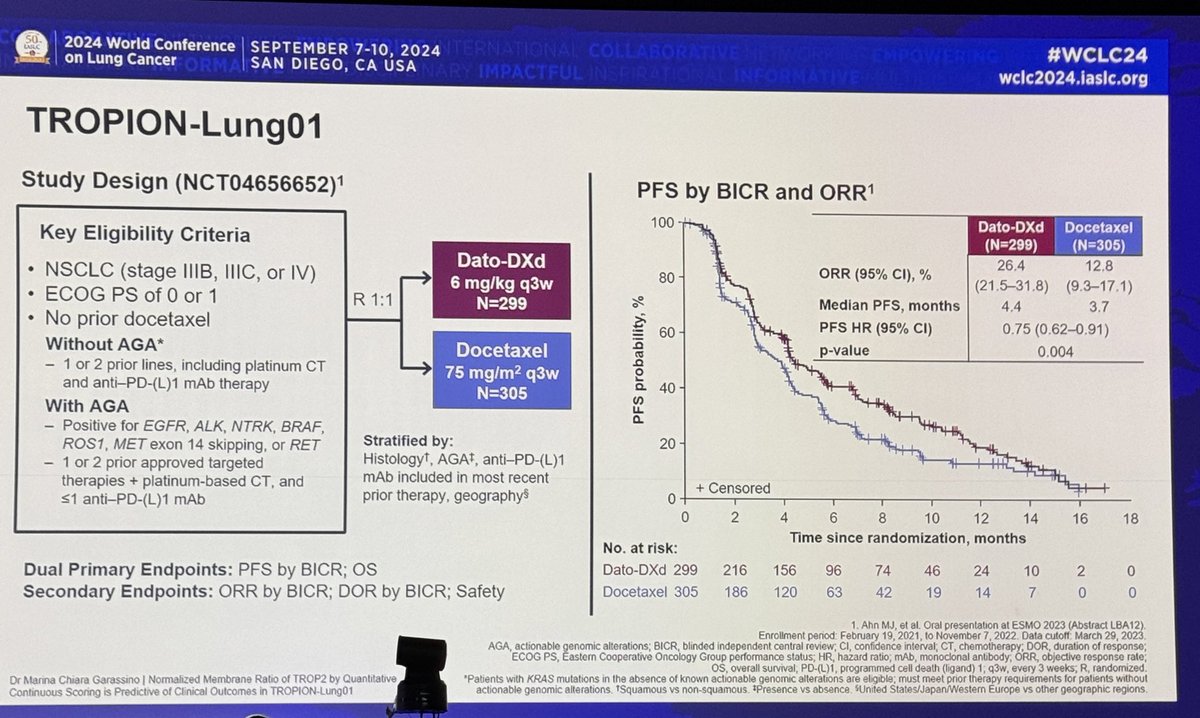
Study design here shows randomization to first-line sintilimab + anlotinib or chemo (with sintilimab at progression). Some concerns about randomization to chemotherapy without immunotherapy in a modern day study. #ESMO22


Baseline characteristics show a fairly high proportion of never smokers. SUNRISE excluded EGFR, ALK, and ROS1 - would like details on testing methods and presence of other drivers. More pts with brain and liver metastases in the sintilimab + anlotinib arm. #ESMO22

Primary endpoint of RR favors sintilimab + anlotinib (50% vs 33%). DOR 16.3 vs 6.2m and PFS HR 0.40. No TRAE leading to discontinuation with sintilimab + anlotinib and overall well tolerated. #ESMO22


Encouraging data - but small study and a bit of an obsolete control arm in this era. Hoping to see more biomarker data from this study and others. #ESMO22

• • •
Missing some Tweet in this thread? You can try to
force a refresh