Dr. @ZPiotrowskaMD presents initial results from the ELIOS trial at #ESMO22 - molecular profiling of #EGFR mutant NSCLC after progression on 1L osimertinib. 


In this study of highly motivated pts at esteemed sites, evaluable paired biopsy at PD only available in 46/115 pts (40%). Interestingly, 75 pts (65%) had paired biopsy but 27 failed NGS (23%). Speaks somewhat to the real world feasibility of a repeat biopsy approach. #ESMO22

Common co-mutations at baseline included TP53, EGFR amp, and CDKN2A loss. Acquired alterations included MET amp, EGFR C797S, ALK fusion, NKX2-1 amp. Mostly mutually exclusive. #ESMO22



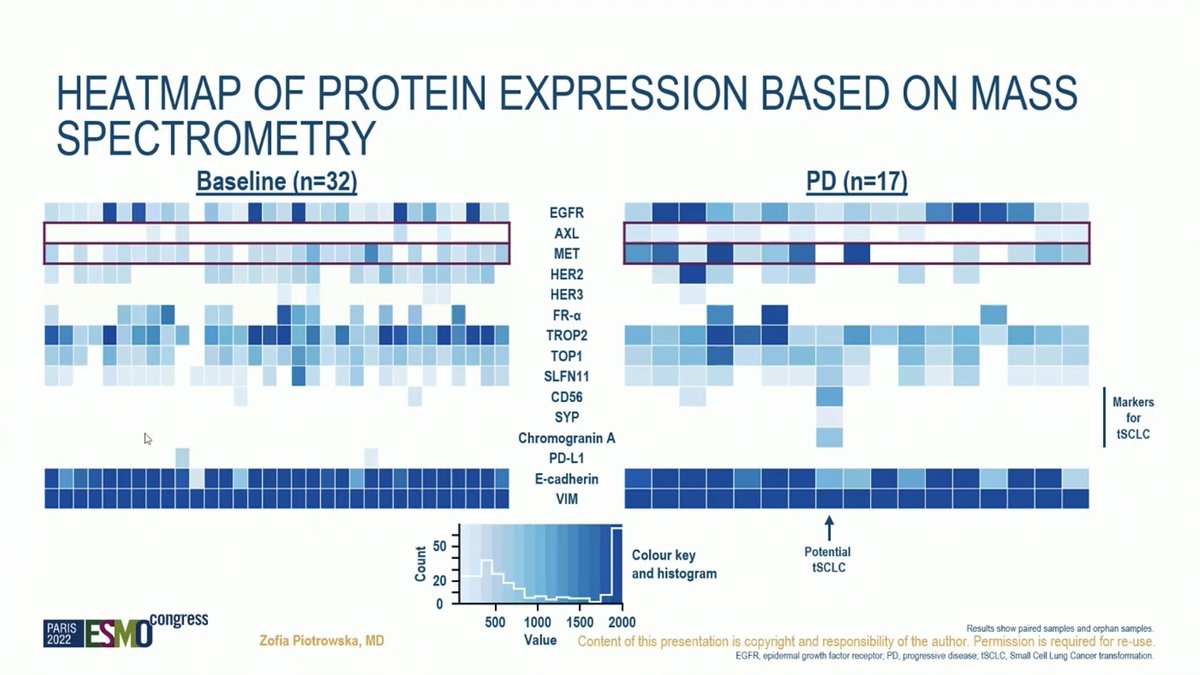
Large subset of acquired resistance remains undefined by genomic analysis. Important proteomic work included on this trial identifies alterations in AXL and MET at progression. #ESMO22


Outcomes with osimertinib as expected. Takeaways from ELIOS include the difficulties in getting paired biopsies at progression for analysis and the frequency of acquired MET amp and EGFR C797S at progression on 1L osimertinib. Await more data including histology. #ESMO22



• • •
Missing some Tweet in this thread? You can try to
force a refresh