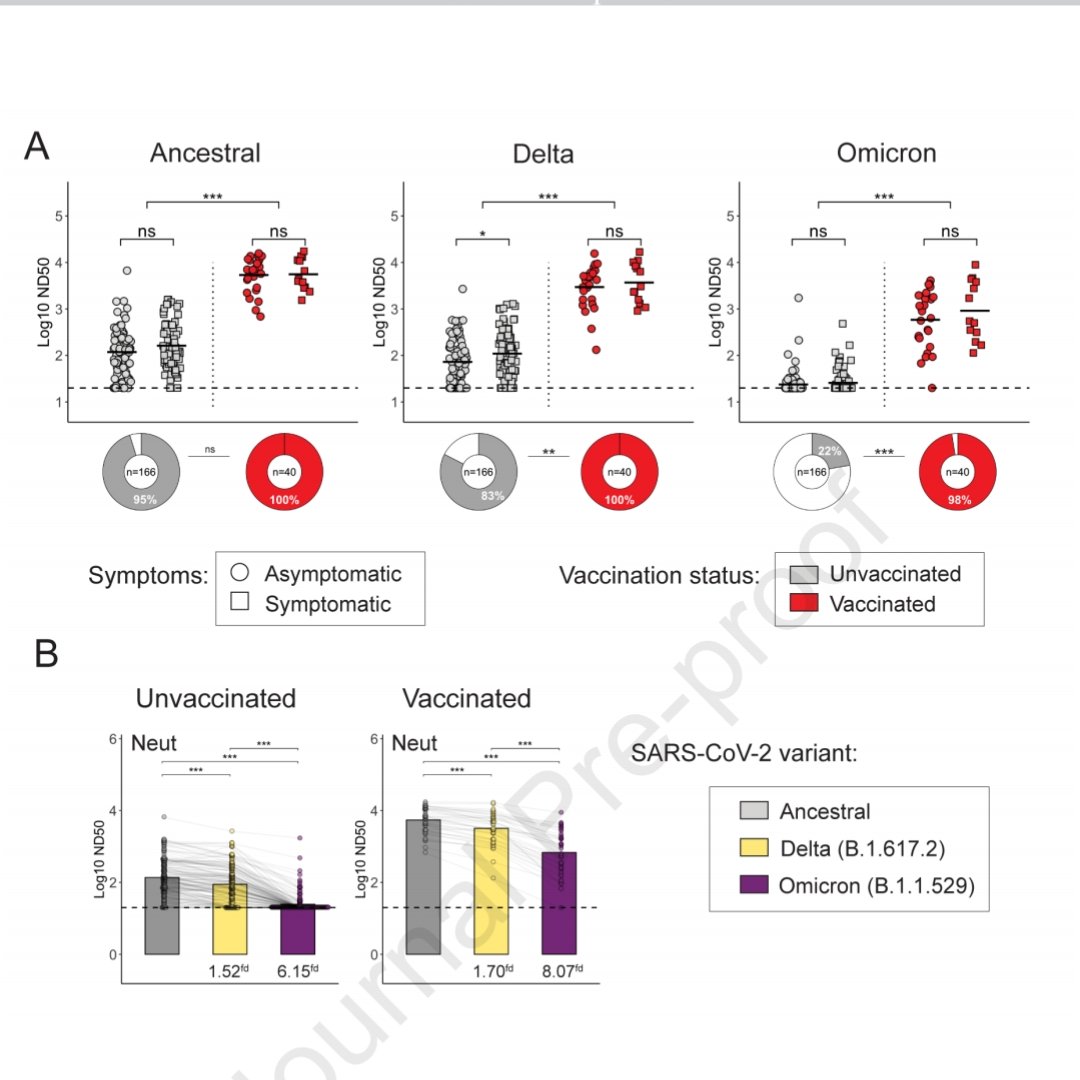
@Sobretutumba @orwell2022 @OS51388957 @mr_Smith_Econ @connolly_s ??? Really??? Isnt this study saying 2 vax+infection is great & u get a great immune response? Thats crazy! If anything adding booster makes it worse as seen in triple vaxed controversial health care worker study where type of prior infection may matter:
https://twitter.com/EphemeralEther/status/1536928712628781057?s=20&t=_-UjeCoutZBJkoSTdkYvbg
@Sobretutumba @orwell2022 @OS51388957 @mr_Smith_Econ @connolly_s What i find interesting about both of these studies is the lack of correlation to symptoms! If increased immune activity (neutralizing, t cells, b cells etc) doesnt change your symptom outcome, what are we measuring & how important is it to overall health outcomes? 

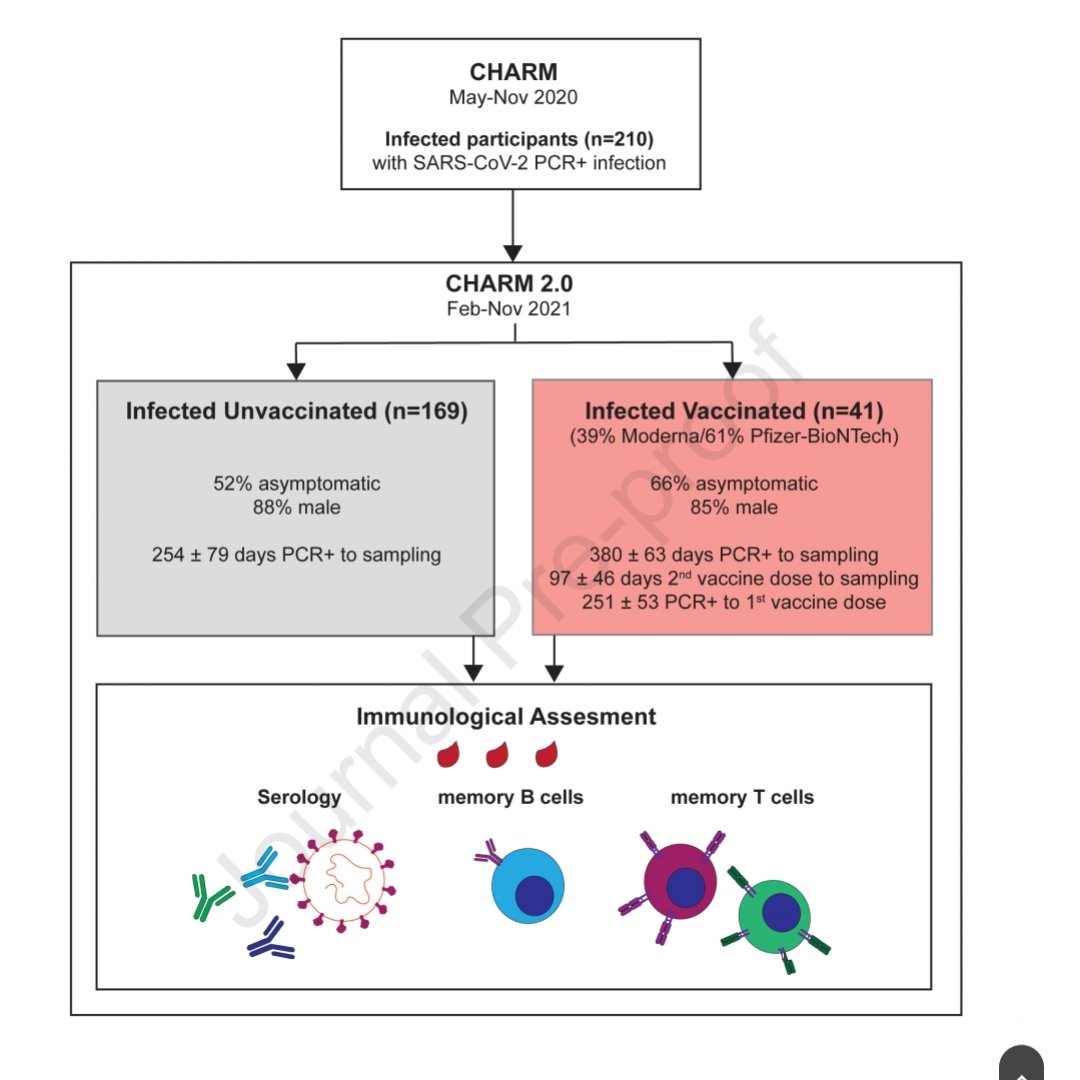
@Sobretutumba @orwell2022 @OS51388957 @mr_Smith_Econ @connolly_s Now of course u could say vaxed had more asymptomatic infx, on the other hand their uneven cohort #s are a caveat: 169 unvaxed vs only 41 vaxed. And if u cant show correlation with your various immune response measurements, it brings more questions than answers, as always ;-)
@Sobretutumba @orwell2022 @OS51388957 @mr_Smith_Econ @connolly_s The discrepancy may be because more details are needed as seen in this paper, where the quality of the stimulated immune cells matter which may actually be less good in vaxed
https://twitter.com/EphemeralEther/status/1570135040863997955?s=20&t=_-UjeCoutZBJkoSTdkYvbg
@Sobretutumba @orwell2022 @OS51388957 @mr_Smith_Econ @connolly_s My takeaway here is the same as from the response attenuation we saw in triple vaxed wuhan+omicron & multiple omicron: over-exposure to spike is bad. The fact that vaxed consistently have a stronger immune response is not necessarily a good thing...
@Sobretutumba @orwell2022 @OS51388957 @mr_Smith_Econ @connolly_s overstimulation, autoimmunity & cytokine storms come to mind. But then again what is the right response? What constitutes as aberrant?
@Sobretutumba @orwell2022 @OS51388957 @mr_Smith_Econ @connolly_s They say in the paper this is good because it will decrease transmission (cuz they cant talk about severe disease in such a young healthy cohort that doesnt need vax for personal health). Yet we see in many places now vaxed having more infx than unvaxed (ontario, canada)
@Sobretutumba @orwell2022 @OS51388957 @mr_Smith_Econ @connolly_s Here is another great thread highlighting how it is previous infection that underlies the protection against transmission NOT vax
https://twitter.com/FSBuchholzer/status/1574692091447615488?s=20&t=_-UjeCoutZBJkoSTdkYvbg
@Sobretutumba @orwell2022 @OS51388957 @mr_Smith_Econ @connolly_s If u look carefully u see how in omicron household contacts uninfected vaxed had even slightly higher rates than uninfected unvaxed...interesting!
https://twitter.com/TijlDeBie/status/1574386887195852802?s=20&t=_-UjeCoutZBJkoSTdkYvbg
@Sobretutumba @orwell2022 @OS51388957 @mr_Smith_Econ @connolly_s i point this out because one must be wary of studies making unsupported claims. They should instead ask: what do our results really show? Or at least measure infection rates & tie them to the immune response! Just saying higher response = less transmission is lazy marketing
• • •
Missing some Tweet in this thread? You can try to
force a refresh