💚Top Ten Slides from day 1 of #BSEcho2022 💚
A thread for all those who echo
1) Should we use the highest beat/signal in AF? Slide shown by Sanjeev Bhattacharyya
1/n
A thread for all those who echo
1) Should we use the highest beat/signal in AF? Slide shown by Sanjeev Bhattacharyya
1/n

2) Peripartum cardiomyopathy - don't miss it and remember need to counsel/risk stratisfy if considering future pregnancies. Slide shown by @BSE_President Claire Colebourn at #BSEcho2022
2/n
2/n

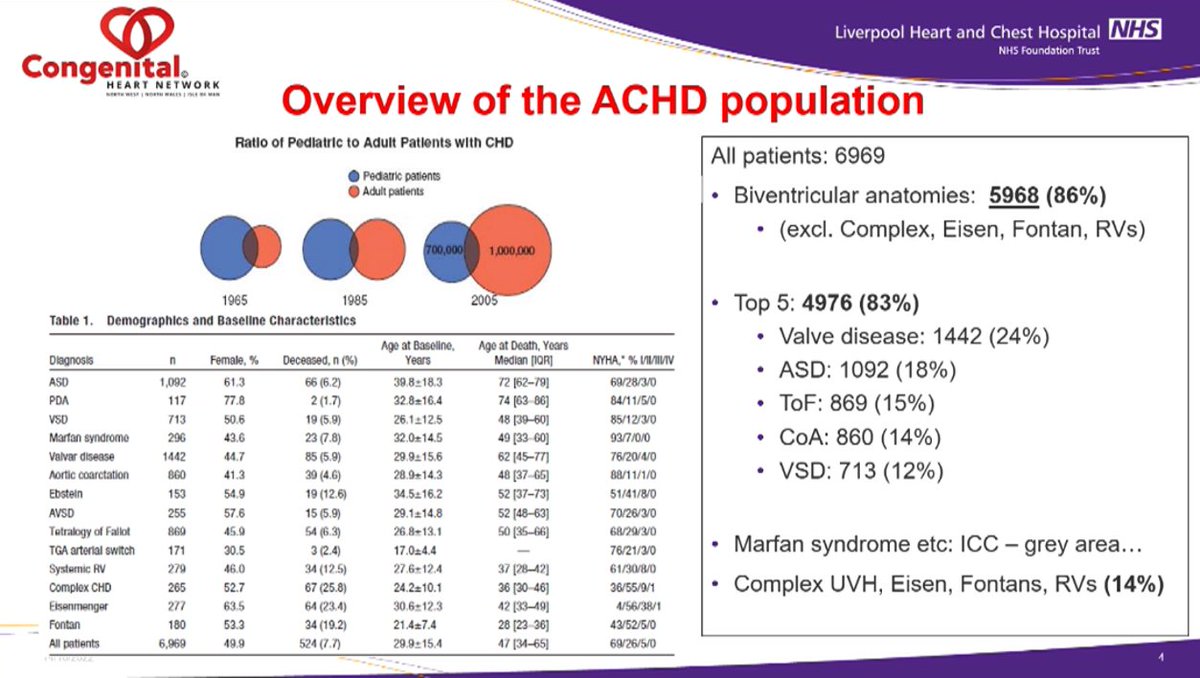
3) The adult ACHD population is larger than the paediatric one, and 86% have biventricular anatomies. Interesting UK data shown by Liam Corbett at #BSEcho2022
3/n
3/n
4) Exercise stress beats dobutamine for assessment of myocardial ischaemia by echo - reminder slide shown by Prof Roxy Senior at #BSEcho2022
4/n
4/n

5) Schematic of how to approach assessment of prosthetic heart valves, shown by Jim Newton at #BSEcho2022
5/n
5/n

6) Patient prosthesis mismatch - table of grading shown by @hothi_sandeep at #BSEcho2022 - note different ranges based on BMI.
6/n
6/n


8) How often should a pt with a known regurgitant lesion and no complications have an echo when pregnant? Slide shown by Steph Curtis at #BSEcho2022
8/n
8/n

9) A recap of the usual association of coronary arteries with echo segments, shown by Wendy Gamblin at #BSEcho2022
9/n
9/n

10) When to routinely echo pts with prosthetic valves - slide shown by @hothi_sandeep at #BSEcho2022
10/n
10/n

It was really hard to choose 10 as there were so many brilliant talks - thanks to all who worked hard to organise #BSEcho2022, and I'm sorry I couldn't be there in person.
@DrDanAugustine @DrEmmaRees @guyll @NavMasani @jwillis82 @nat_echo @The_echo_lady @Faffandtwig
11/11
@DrDanAugustine @DrEmmaRees @guyll @NavMasani @jwillis82 @nat_echo @The_echo_lady @Faffandtwig
11/11
Apologies to @wendyjg75 as I added an extra letter to her name 😳
• • •
Missing some Tweet in this thread? You can try to
force a refresh