Cardiologist- Heart Failure & Advanced Echo; Digital Health - Topol Digital Fellow 2019/2020; Data and process optimisation
 1) CTCA with FFR in 50 pts with type 2 MI showed 92% had CAD, and 26% had obstructive disease, supporting use of aspirin and lipid lowering therapy in pts with T2MI.
1) CTCA with FFR in 50 pts with type 2 MI showed 92% had CAD, and 26% had obstructive disease, supporting use of aspirin and lipid lowering therapy in pts with T2MI.
 1) MITRAL trial outcome looking at 5 yr survival after transcatheter Sapien valve use in mitral position
1) MITRAL trial outcome looking at 5 yr survival after transcatheter Sapien valve use in mitral position
 1) Use of MitraClip in pts with secondary MR – COAPT-PAS, US prospective observational study of 5000 pts, showed significantly⬇️mortality & HF hospitalisation compared to pts in COAPT-RCT GDMT arm ( 33.7% Vs 46.2%)
1) Use of MitraClip in pts with secondary MR – COAPT-PAS, US prospective observational study of 5000 pts, showed significantly⬇️mortality & HF hospitalisation compared to pts in COAPT-RCT GDMT arm ( 33.7% Vs 46.2%)  1) At 3 months post PCI, the TWILIGHT RCT published in @JACCJournals showed ticagrelor monotherapy compared to continued DAPT (ticagrelor and aspirin) resulted in lower bleeding risk with no increase in ischaemic risk
1) At 3 months post PCI, the TWILIGHT RCT published in @JACCJournals showed ticagrelor monotherapy compared to continued DAPT (ticagrelor and aspirin) resulted in lower bleeding risk with no increase in ischaemic risk 1) Use of hs-cTnI to risk stratify pts with chronic CAD: 1 in 25 had trop >99th percentile & these pts had a 4x ⬆️risk MI/CV death vs pts <5ng/L. -MICA study in @JACCJournals
1) Use of hs-cTnI to risk stratify pts with chronic CAD: 1 in 25 had trop >99th percentile & these pts had a 4x ⬆️risk MI/CV death vs pts <5ng/L. -MICA study in @JACCJournals  2) Summary slide of drugs that may be used in shock plotted on a scale of inotropy and vasoconstriction.
2) Summary slide of drugs that may be used in shock plotted on a scale of inotropy and vasoconstriction.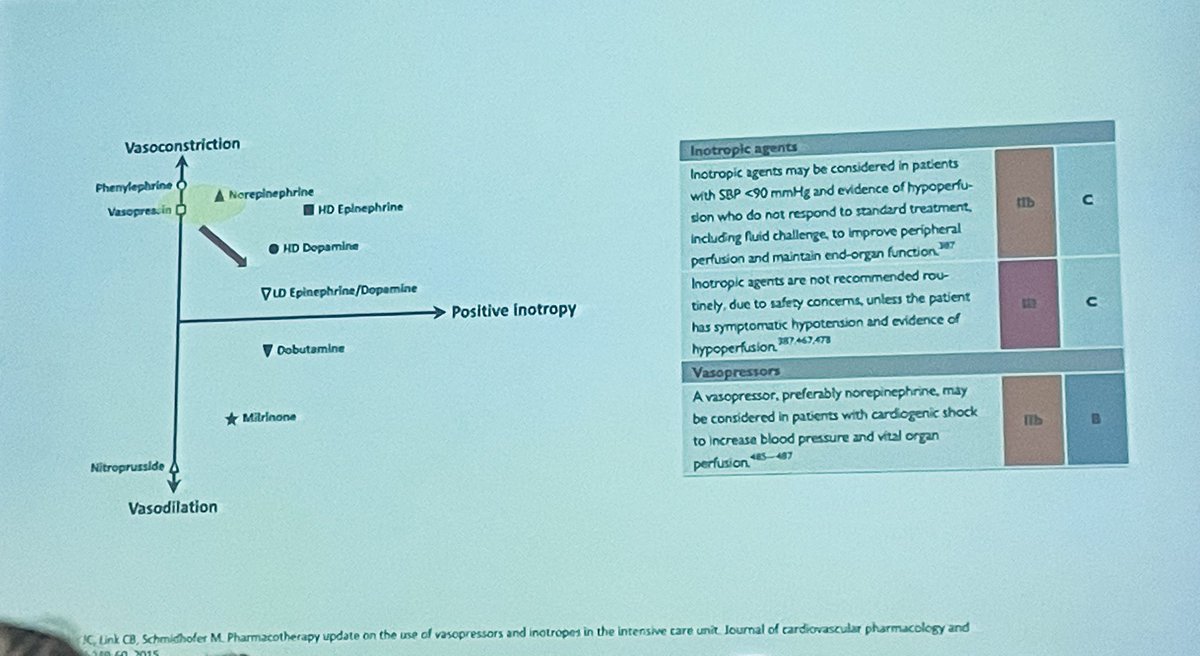
 2) Peripartum cardiomyopathy - don't miss it and remember need to counsel/risk stratisfy if considering future pregnancies. Slide shown by @BSE_President Claire Colebourn at #BSEcho2022
2) Peripartum cardiomyopathy - don't miss it and remember need to counsel/risk stratisfy if considering future pregnancies. Slide shown by @BSE_President Claire Colebourn at #BSEcho2022


 2) Revascularization with PCI does not improve event-free survival in pts with severe LVSD over OMT alone
2) Revascularization with PCI does not improve event-free survival in pts with severe LVSD over OMT alone 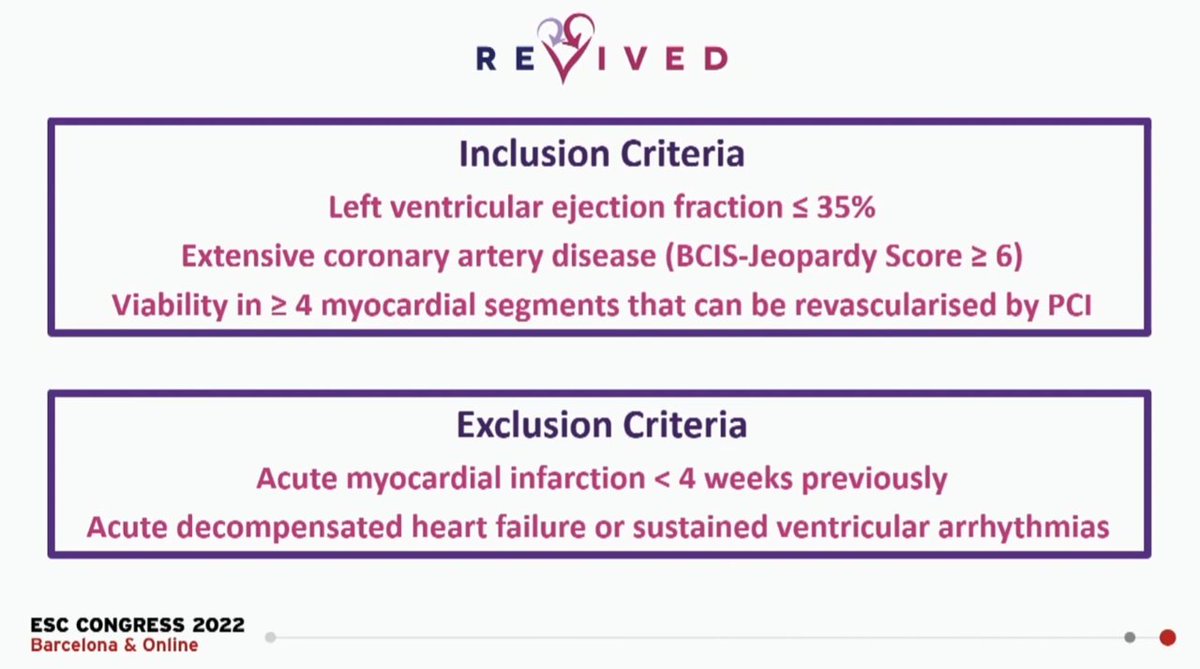



 The #ESCCongress session started with @FudimMarat discussing how it worked – explaining how pts with HF have poor baroreflex sensitivity, that baroreflex down-regulation is related to worse HF symptoms & barostim provided chronic improvement in muscle sym nerve activity
The #ESCCongress session started with @FudimMarat discussing how it worked – explaining how pts with HF have poor baroreflex sensitivity, that baroreflex down-regulation is related to worse HF symptoms & barostim provided chronic improvement in muscle sym nerve activity 



 Indications for referral for surgery for severe asymptomatic AS:
Indications for referral for surgery for severe asymptomatic AS:
 2) A more aggressive BP target (110 to 130 Vs 130 to 150) in elderly patients resulted in lower rates of cardiovascular events
2) A more aggressive BP target (110 to 130 Vs 130 to 150) in elderly patients resulted in lower rates of cardiovascular events 



 1)The indications for surgery in severe asym AR have changed
1)The indications for surgery in severe asym AR have changed
 2) SGLT2i in addition to standard HF treatment significantly ⬇️CV death, including in non-diabetic pts
2) SGLT2i in addition to standard HF treatment significantly ⬇️CV death, including in non-diabetic pts 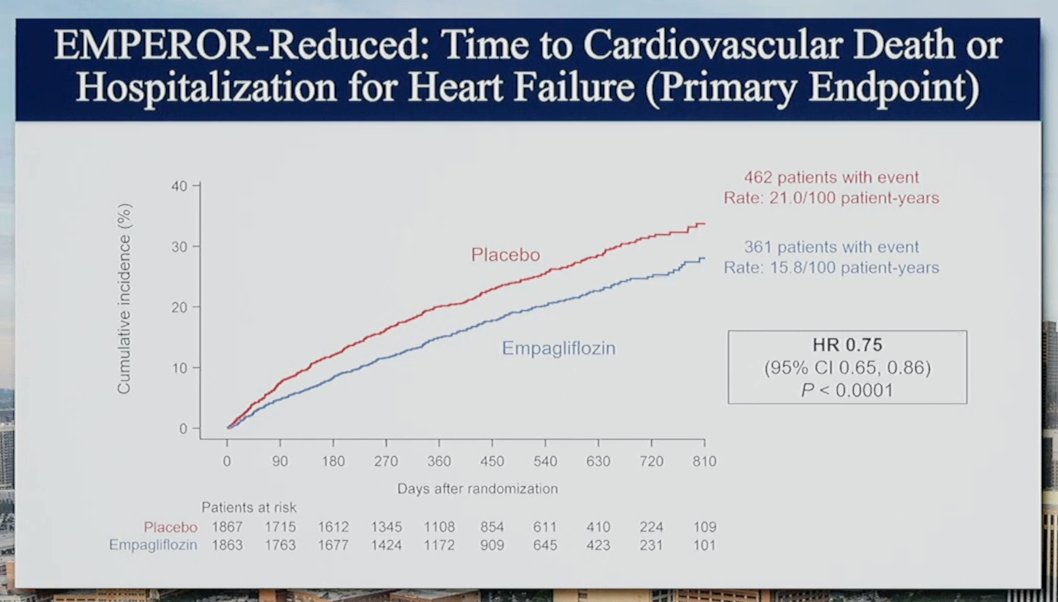
 To start with the basics: the size of the aortic root varies based on sex, height, weight and age, so these details are required to put a basic figure into context.
To start with the basics: the size of the aortic root varies based on sex, height, weight and age, so these details are required to put a basic figure into context. 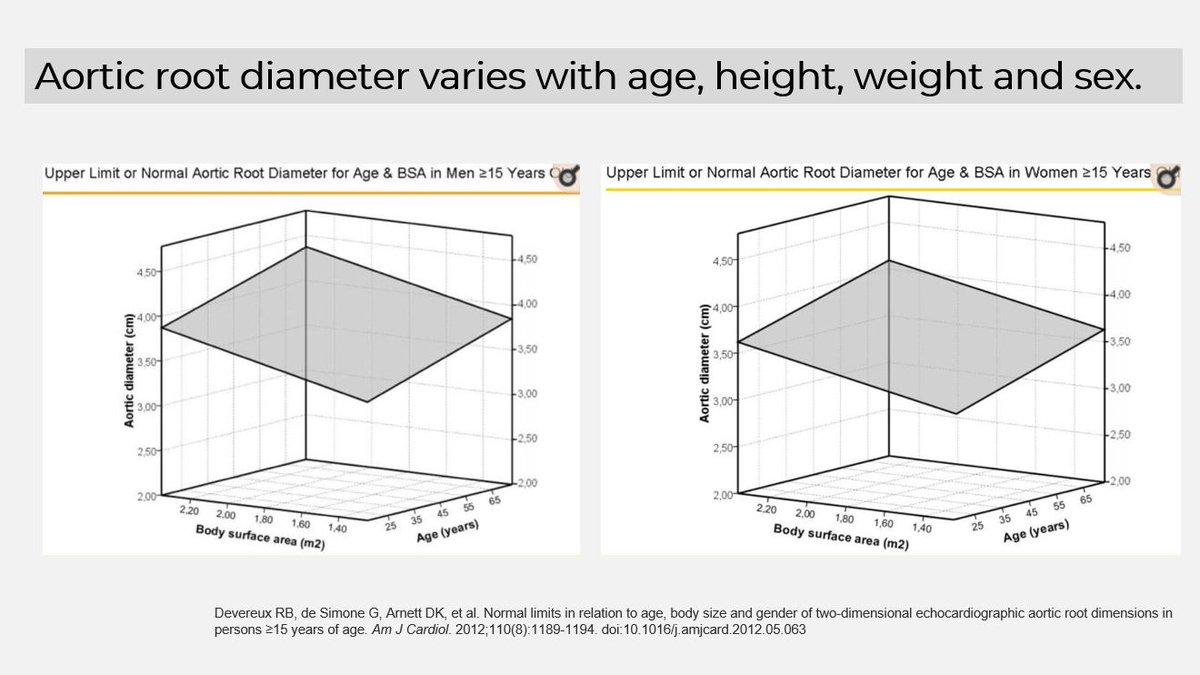
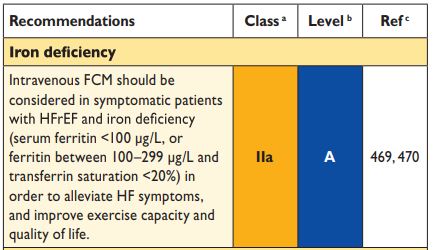
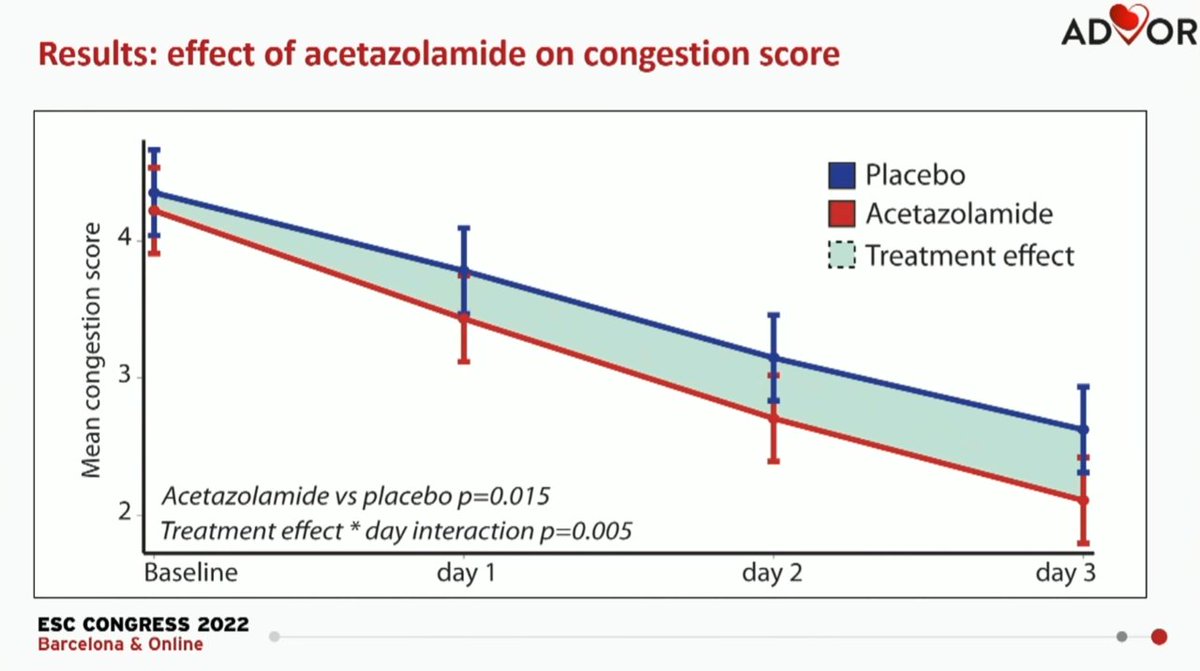
 ESC guidelines recommend IV iron in patients with HFrEF (EF<40%), Hb <15g/dL and iron deficiency, which is defined as:
ESC guidelines recommend IV iron in patients with HFrEF (EF<40%), Hb <15g/dL and iron deficiency, which is defined as: