
@TumorBoardTues 1/17 #TumorBoardTuesday #LungCancer #OncTwitter
42yo 👨🏽💼
PMH: never smoker
persistent cough
🩻PET/CT: 3.5 cm mass LLL & bulky, coalescing LNs in L hilum & mediastinum (AP 🪟, subcarinal, bilat paratracheal, supraclav)
Axillary LNs
🦴multi bony mets
🫀small pericardial effusion
42yo 👨🏽💼
PMH: never smoker
persistent cough
🩻PET/CT: 3.5 cm mass LLL & bulky, coalescing LNs in L hilum & mediastinum (AP 🪟, subcarinal, bilat paratracheal, supraclav)
Axillary LNs
🦴multi bony mets
🫀small pericardial effusion
@TumorBoardTues 2/17 #TumorBoardTuesday #LungCancer #NSCLC
🫁🎥Mediastinoscopy shows adenocarcinoma with signet rings.
🔬 ALK IHC positive
🐟 FISH positive
🧬 PDL1 = 0
🤨What’s your recommended initial therapy:
🫁🎥Mediastinoscopy shows adenocarcinoma with signet rings.
🔬 ALK IHC positive
🐟 FISH positive
🧬 PDL1 = 0
🤨What’s your recommended initial therapy:
@TumorBoardTues 3/17 #TumorBoardTuesday #LCSM
🧲MRI: Brain shows 4 CNS mets in frontal lobes & cerebellum
📏 = 13, 10, 8 and 4 mm
💧No edema
🧠 no neuro symptoms
🤨 Does the presence of CNS mets change your 1st line recommendation?
A = alectinib
B = brigatinib
L = lorlatinib
🧲MRI: Brain shows 4 CNS mets in frontal lobes & cerebellum
📏 = 13, 10, 8 and 4 mm
💧No edema
🧠 no neuro symptoms
🤨 Does the presence of CNS mets change your 1st line recommendation?
A = alectinib
B = brigatinib
L = lorlatinib
@TumorBoardTues 4/17 #TumorBoardTuesday
Plot twist!
👨🏽💼seen when criz only 1L ALK TKI avail
👉🏽got WBRT (criz poor CNS penetration)
👨🏽💼treated with criz 250mg BID
👍🏽initial response in all sites➡️multifocal 🧠progress after 14 mo
👨🏽💼2L alectinib 600mg BID➡️good response
📚pubmed.ncbi.nlm.nih.gov/27863201/
Plot twist!
👨🏽💼seen when criz only 1L ALK TKI avail
👉🏽got WBRT (criz poor CNS penetration)
👨🏽💼treated with criz 250mg BID
👍🏽initial response in all sites➡️multifocal 🧠progress after 14 mo
👨🏽💼2L alectinib 600mg BID➡️good response
📚pubmed.ncbi.nlm.nih.gov/27863201/
@TumorBoardTues 5/17 #TumorBoardTuesday
👩🏻⚕️Mini tweetorial 1
📌ALK NSCLC
✅Occur in 5% of #NSCLC, primarily adenocarcinoma
✅More common in non-smokers, younger patients
✅About 30% with brain mets at the time of diagnosis
📚 pubmed.ncbi.nlm.nih.gov/23401436/
📚 pubmed.ncbi.nlm.nih.gov/36257531/
👩🏻⚕️Mini tweetorial 1
📌ALK NSCLC
✅Occur in 5% of #NSCLC, primarily adenocarcinoma
✅More common in non-smokers, younger patients
✅About 30% with brain mets at the time of diagnosis
📚 pubmed.ncbi.nlm.nih.gov/23401436/
📚 pubmed.ncbi.nlm.nih.gov/36257531/
@TumorBoardTues 6/17 #TumorBoardTuesday
👩🏻⚕️ Mini tweetorial 2
📌ALK #NSCLC
What’s best diagnostic?
🧪‘Break apart’ FISH assay is gold standard, but requires ⬆️expertise to interpret
🧪IHC is now ✅ equivalent to 🐟
🔹IHC recommended in latest CAP/IASLC/AMP guidelines as 🐟 alternative
👩🏻⚕️ Mini tweetorial 2
📌ALK #NSCLC
What’s best diagnostic?
🧪‘Break apart’ FISH assay is gold standard, but requires ⬆️expertise to interpret
🧪IHC is now ✅ equivalent to 🐟
🔹IHC recommended in latest CAP/IASLC/AMP guidelines as 🐟 alternative

@TumorBoardTues @ALKLungCancer @EricBernicker @MurryWynes @JessicaJLinMD @StephenVLiu @n8pennell @HenningWillers @oncoOuLungCA @CharuAggarwalMD @MLadanyi 7/17 #TumorBoardTuesday
👩🏻⚕️ Mini tweetorial 3
📌ALK NSCLC
NGS also🏆at dx ALK, esp if using RNA assay
🤔No DNA 🧪can ✔️ all possible breakpoints
💡RNA coding elements <2% ALK gene➡️can be covered 💯
RNA 🧪can🔎all variants regardless of fusion partner
📚 tinyurl.com/yefw7ndz
👩🏻⚕️ Mini tweetorial 3
📌ALK NSCLC
NGS also🏆at dx ALK, esp if using RNA assay
🤔No DNA 🧪can ✔️ all possible breakpoints
💡RNA coding elements <2% ALK gene➡️can be covered 💯
RNA 🧪can🔎all variants regardless of fusion partner
📚 tinyurl.com/yefw7ndz
@TumorBoardTues @ALKLungCancer @EricBernicker @MurryWynes @JessicaJLinMD @StephenVLiu @n8pennell @HenningWillers @oncoOuLungCA @CharuAggarwalMD @MLadanyi 8/17 #TumorBoardTuesday #LCSM
👩🏻⚕️ Mini tweetorial 4
📌ALK treatment
📍Proof of concept🎯w/multi-kinase crizotinib
📍Next specific 2nd-gen ALK TKIs 🛬
📍1st up: ceritinib. Not freq used (⬆️tox)
✨ASCEND4: 1L cerit v plat doublet chemo: med PFS 17 v 8 mo
📚tinyurl.com/4wewx78c
👩🏻⚕️ Mini tweetorial 4
📌ALK treatment
📍Proof of concept🎯w/multi-kinase crizotinib
📍Next specific 2nd-gen ALK TKIs 🛬
📍1st up: ceritinib. Not freq used (⬆️tox)
✨ASCEND4: 1L cerit v plat doublet chemo: med PFS 17 v 8 mo
📚tinyurl.com/4wewx78c


@TumorBoardTues @ALKLungCancer @EricBernicker @MurryWynes @JessicaJLinMD @StephenVLiu @n8pennell @HenningWillers @oncoOuLungCA @CharuAggarwalMD @MLadanyi @bensolomon1 @CoreyLangerMD @RamalingamMD @triparnasen @HwakeleeMD @JulieBrahmer @NarjustFlorezMD @HosseinBorghaei @benlevylungdoc @BrendonStilesMD 9/17 #TumorBoardTuesday
👩🏻⚕️Mini tweetorial 5
ALK treatment
📌Alectinib
✅well tolerated
✅👍🏽 CNS activity
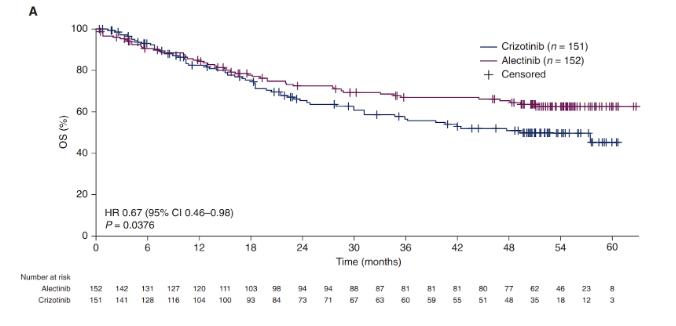
✨ALEX trial: 1L alec v criz: med PFS 35 v 11 mo
Med OS still NR; 5yr landmark OS: 63% v 46%
⚡️CNS protection marked⚡️
📚@peters_solange NEJM 2017
📚@tonymok9 AnnOnc 2020
👩🏻⚕️Mini tweetorial 5
ALK treatment
📌Alectinib
✅well tolerated
✅👍🏽 CNS activity
✨ALEX trial: 1L alec v criz: med PFS 35 v 11 mo
Med OS still NR; 5yr landmark OS: 63% v 46%
⚡️CNS protection marked⚡️
📚@peters_solange NEJM 2017
📚@tonymok9 AnnOnc 2020

@TumorBoardTues @ALKLungCancer @EricBernicker @MurryWynes @JessicaJLinMD @StephenVLiu @n8pennell @HenningWillers @oncoOuLungCA @CharuAggarwalMD @MLadanyi @bensolomon1 @CoreyLangerMD @RamalingamMD @triparnasen @HwakeleeMD @JulieBrahmer @NarjustFlorezMD @HosseinBorghaei @benlevylungdoc @BrendonStilesMD @peters_solange @TonyMok9 @JustinGainor @JackWestMD @christine_lovly @IbiayiMD @Latinamd @Joshua_Reuss @JuliaRotow @ReckampK @AngelQinMD @DocSacher 10/17 #TumorBoardTuesday #LCSM
👩🏻⚕️ Mini tweetorial 6
ALK treatment
📌Alectinib
✨ALEX trial✨
♦️For those w/o prior CNS mets, CNS PD at 1 year:
🔸31% on crizotinib
💥only 5% on alectinib
📚@gadgeel @Annals_Oncology 2018
👩🏻⚕️ Mini tweetorial 6
ALK treatment
📌Alectinib
✨ALEX trial✨
♦️For those w/o prior CNS mets, CNS PD at 1 year:
🔸31% on crizotinib
💥only 5% on alectinib
📚@gadgeel @Annals_Oncology 2018

@TumorBoardTues @ALKLungCancer @EricBernicker @MurryWynes @JessicaJLinMD @StephenVLiu @n8pennell @HenningWillers @oncoOuLungCA @CharuAggarwalMD @MLadanyi @bensolomon1 @CoreyLangerMD @RamalingamMD @triparnasen @HwakeleeMD @JulieBrahmer @NarjustFlorezMD @HosseinBorghaei @benlevylungdoc @BrendonStilesMD @peters_solange @TonyMok9 @JustinGainor @JackWestMD @christine_lovly @IbiayiMD @Latinamd @Joshua_Reuss @JuliaRotow @ReckampK @AngelQinMD @DocSacher @gadgeel @Annals_Oncology @ConorSteuerMD @BrunaPellini @LeXiuning @LaurenByersMD @DrSteveMartin @ZPiotrowskaMD @KCArbourMD @ValsamoA @maryjofidlerMD @Jia_Luo 11/17 #TumorBoardTuesday
👩🏻⚕️Mini tweetorial 7
ALK treatment
📌Brigatinib
✅well tolerated
✅dose starts 90mg x 1wk, then ⬆️180mg to avoid rare but serious pneumonitis
✅excellent CNS penetration
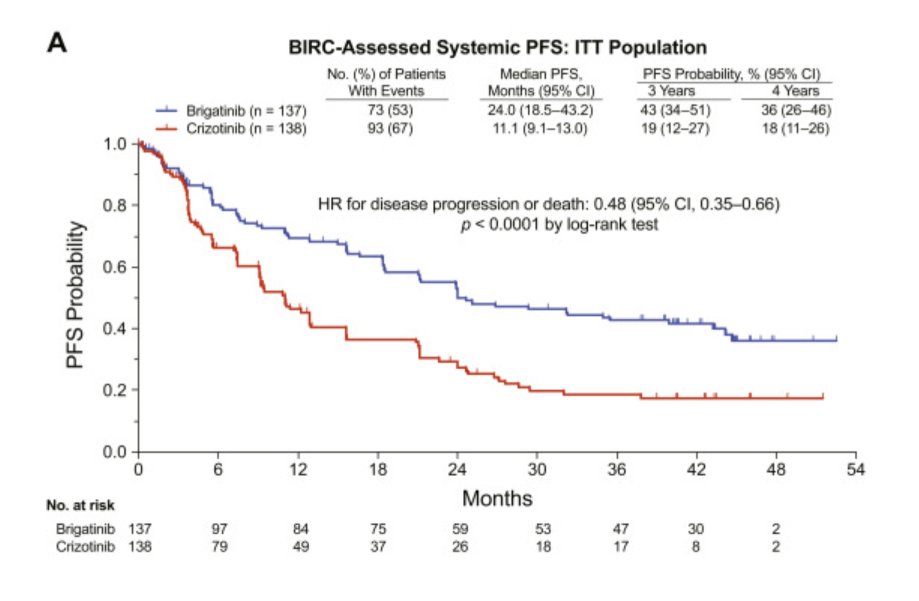
✨ALTA-1L trial, 1st line brig vs criz had med PFS 24 vs 11 mo
📚Camidge JTO 2021
👩🏻⚕️Mini tweetorial 7
ALK treatment
📌Brigatinib
✅well tolerated
✅dose starts 90mg x 1wk, then ⬆️180mg to avoid rare but serious pneumonitis
✅excellent CNS penetration
✨ALTA-1L trial, 1st line brig vs criz had med PFS 24 vs 11 mo
📚Camidge JTO 2021
@TumorBoardTues @ALKLungCancer @EricBernicker @MurryWynes @JessicaJLinMD @StephenVLiu @n8pennell @HenningWillers @oncoOuLungCA @CharuAggarwalMD @MLadanyi @bensolomon1 @CoreyLangerMD @RamalingamMD @triparnasen @HwakeleeMD @JulieBrahmer @NarjustFlorezMD @HosseinBorghaei @benlevylungdoc @BrendonStilesMD @peters_solange @TonyMok9 @JustinGainor @JackWestMD @christine_lovly @IbiayiMD @Latinamd @Joshua_Reuss @JuliaRotow @ReckampK @AngelQinMD @DocSacher @gadgeel @Annals_Oncology @ConorSteuerMD @BrunaPellini @LeXiuning @LaurenByersMD @DrSteveMartin @ZPiotrowskaMD @KCArbourMD @ValsamoA @maryjofidlerMD @Jia_Luo @collin_blakely @BeccaHeistMD @ryangentzler 12/17 #TumorBoardTuesday
Back to our case🔎
👨🏽💼After 3 years on alectinib, cancer progressed
💉Bx = new ALK I1171N ➡️ patient rx’d lorlatinib
🤔Different sensitivity of each TKI to each ALK resistance mutation was mapped in 💫 landmark 📚@JustinGainor @CD_AACR paper.
Back to our case🔎
👨🏽💼After 3 years on alectinib, cancer progressed
💉Bx = new ALK I1171N ➡️ patient rx’d lorlatinib
🤔Different sensitivity of each TKI to each ALK resistance mutation was mapped in 💫 landmark 📚@JustinGainor @CD_AACR paper.

@TumorBoardTues @ALKLungCancer @EricBernicker @MurryWynes @JessicaJLinMD @StephenVLiu @n8pennell @HenningWillers @oncoOuLungCA @CharuAggarwalMD @MLadanyi @bensolomon1 @CoreyLangerMD @RamalingamMD @triparnasen @HwakeleeMD @JulieBrahmer @NarjustFlorezMD @HosseinBorghaei @benlevylungdoc @BrendonStilesMD @peters_solange @TonyMok9 @JustinGainor @JackWestMD @christine_lovly @IbiayiMD @Latinamd @Joshua_Reuss @JuliaRotow @ReckampK @AngelQinMD @DocSacher @gadgeel @Annals_Oncology @ConorSteuerMD @BrunaPellini @LeXiuning @LaurenByersMD @DrSteveMartin @ZPiotrowskaMD @KCArbourMD @ValsamoA @maryjofidlerMD @Jia_Luo @collin_blakely @BeccaHeistMD @ryangentzler @CD_AACR 13/17 #TumorBoardTuesday #LCSM
👩🏻⚕️Mini tweetorial 8
📌Lorlatinib: 3rd gen TKI designed to ⬆️🧠 penetration
📍Hits ++ resistance mutations 🥅, incl G1202R, which 🚫 respond to any other ALK TKI
📚Shaw @JCO_ASCO 2019
📍But ⬆️ side effects > 2nd gens: ⬆️lipids, edema, CNS 🔺's
👩🏻⚕️Mini tweetorial 8
📌Lorlatinib: 3rd gen TKI designed to ⬆️🧠 penetration
📍Hits ++ resistance mutations 🥅, incl G1202R, which 🚫 respond to any other ALK TKI
📚Shaw @JCO_ASCO 2019
📍But ⬆️ side effects > 2nd gens: ⬆️lipids, edema, CNS 🔺's

@TumorBoardTues @ALKLungCancer @EricBernicker @MurryWynes @JessicaJLinMD @StephenVLiu @n8pennell @HenningWillers @oncoOuLungCA @CharuAggarwalMD @MLadanyi @bensolomon1 @CoreyLangerMD @RamalingamMD @triparnasen @HwakeleeMD @JulieBrahmer @NarjustFlorezMD @HosseinBorghaei @benlevylungdoc @BrendonStilesMD @peters_solange @TonyMok9 @JustinGainor @JackWestMD @christine_lovly @IbiayiMD @Latinamd @Joshua_Reuss @JuliaRotow @ReckampK @AngelQinMD @DocSacher @gadgeel @Annals_Oncology @ConorSteuerMD @BrunaPellini @LeXiuning @LaurenByersMD @DrSteveMartin @ZPiotrowskaMD @KCArbourMD @ValsamoA @maryjofidlerMD @Jia_Luo @collin_blakely @BeccaHeistMD 14/17 #TumorBoardTuesday
👩🏻⚕️Mini tweetorial 9
📌Lorlatinib: 1st line!
✨CROWN trial: 1L lorlat v criz: med PFS NR v 9.3 mo
📚Shaw @NEJM 2020
🤔Hard to compare across trials 🤷🏽♀️💭wish we had ℹ️ on 1L lorl vs alec
📚@bensolomon1 updated data @JCO_ASCO 2022: 12mo🧠PD 8 v 58%
👩🏻⚕️Mini tweetorial 9
📌Lorlatinib: 1st line!
✨CROWN trial: 1L lorlat v criz: med PFS NR v 9.3 mo
📚Shaw @NEJM 2020
🤔Hard to compare across trials 🤷🏽♀️💭wish we had ℹ️ on 1L lorl vs alec
📚@bensolomon1 updated data @JCO_ASCO 2022: 12mo🧠PD 8 v 58%


@TumorBoardTues @ALKLungCancer @EricBernicker @MurryWynes @JessicaJLinMD @StephenVLiu @n8pennell @HenningWillers @oncoOuLungCA @CharuAggarwalMD @MLadanyi @bensolomon1 @CoreyLangerMD @RamalingamMD @triparnasen @HwakeleeMD @JulieBrahmer @NarjustFlorezMD @HosseinBorghaei @benlevylungdoc @BrendonStilesMD @peters_solange @TonyMok9 @JustinGainor @JackWestMD @christine_lovly @IbiayiMD @Latinamd @Joshua_Reuss @JuliaRotow @ReckampK @AngelQinMD @DocSacher @gadgeel @Annals_Oncology @ConorSteuerMD @BrunaPellini @LeXiuning @LaurenByersMD @DrSteveMartin @ZPiotrowskaMD @KCArbourMD @ValsamoA @maryjofidlerMD @Jia_Luo @collin_blakely @BeccaHeistMD @NEJM @JCO_ASCO 15/17 #TumorBoardTuesday
Back to case🔎
👨🏽💼✅ lorlatinib x 3 yrs 🗓️
Then oligoPD in adrenal
Bx: new MET amp
📍Bypass (off-target) MET amp occurs in ALK
📚@IbiayiMD CCR 2022 tinyurl.com/2armc4nj
👨🏽💼had 1 PD site only ➡️local ablative rx ⚡️& cont lorlat
🤷🏽♀️Maybe criz in future🔮
Back to case🔎
👨🏽💼✅ lorlatinib x 3 yrs 🗓️
Then oligoPD in adrenal
Bx: new MET amp
📍Bypass (off-target) MET amp occurs in ALK
📚@IbiayiMD CCR 2022 tinyurl.com/2armc4nj
👨🏽💼had 1 PD site only ➡️local ablative rx ⚡️& cont lorlat
🤷🏽♀️Maybe criz in future🔮
@TumorBoardTues @ALKLungCancer @EricBernicker @MurryWynes @JessicaJLinMD @StephenVLiu @n8pennell @HenningWillers @oncoOuLungCA @CharuAggarwalMD @MLadanyi @bensolomon1 @CoreyLangerMD @RamalingamMD @triparnasen @HwakeleeMD @JulieBrahmer @NarjustFlorezMD @HosseinBorghaei @benlevylungdoc @BrendonStilesMD @peters_solange @TonyMok9 @JustinGainor @JackWestMD @christine_lovly @IbiayiMD @Latinamd @Joshua_Reuss @JuliaRotow @ReckampK @AngelQinMD @DocSacher @gadgeel @Annals_Oncology @ConorSteuerMD @BrunaPellini @LeXiuning @LaurenByersMD @DrSteveMartin @ZPiotrowskaMD @KCArbourMD @ValsamoA @maryjofidlerMD @Jia_Luo @collin_blakely @BeccaHeistMD @NEJM @JCO_ASCO 16/17 #TumorBoardTuesday #LCAM
🙏🏽Pt continues to do well x many years 🗓️
🔮More options in the future:
🔸Target the MET amp if it recurs
🔹Chemotherapy
🔸Experimental approaches: ALK + other combos, next gen TKIs, ADCs, modulating immune system
🙏🏽Pt continues to do well x many years 🗓️
🔮More options in the future:
🔸Target the MET amp if it recurs
🔹Chemotherapy
🔸Experimental approaches: ALK + other combos, next gen TKIs, ADCs, modulating immune system
@TumorBoardTues @ALKLungCancer @EricBernicker @MurryWynes @JessicaJLinMD @StephenVLiu @n8pennell @HenningWillers @oncoOuLungCA @CharuAggarwalMD @MLadanyi @bensolomon1 @CoreyLangerMD @RamalingamMD @triparnasen @HwakeleeMD @JulieBrahmer @NarjustFlorezMD @HosseinBorghaei @benlevylungdoc @BrendonStilesMD @peters_solange @TonyMok9 @JustinGainor @JackWestMD @christine_lovly @IbiayiMD @Latinamd @Joshua_Reuss @JuliaRotow @ReckampK @AngelQinMD @DocSacher @gadgeel @Annals_Oncology @ConorSteuerMD @BrunaPellini @LeXiuning @LaurenByersMD @DrSteveMartin @ZPiotrowskaMD @KCArbourMD @ValsamoA @maryjofidlerMD @Jia_Luo @collin_blakely @BeccaHeistMD @NEJM @JCO_ASCO 17/17 #TumorBoardTuesday
Biggest⬇️👨🏽💼QoL has been long term WBRT tox 😢
📌NGS at dx and HOLD WBRT and IO until ✅genotype is known is🔑
Thanks for joining! 🙏🏽Unbelievably proud of @MGHThoracicOnc team for 15y+ ALK research🙌🏽
🚨Anyone with 🫁 can get #LungCancer Nov is #LCAM
Biggest⬇️👨🏽💼QoL has been long term WBRT tox 😢
📌NGS at dx and HOLD WBRT and IO until ✅genotype is known is🔑
Thanks for joining! 🙏🏽Unbelievably proud of @MGHThoracicOnc team for 15y+ ALK research🙌🏽
🚨Anyone with 🫁 can get #LungCancer Nov is #LCAM

@TumorBoardTues @ALKLungCancer @EricBernicker @MurryWynes @JessicaJLinMD @StephenVLiu @n8pennell @HenningWillers @oncoOuLungCA @CharuAggarwalMD @MLadanyi @bensolomon1 @CoreyLangerMD @RamalingamMD @triparnasen @HwakeleeMD @JulieBrahmer @NarjustFlorezMD @HosseinBorghaei @benlevylungdoc @BrendonStilesMD @peters_solange @TonyMok9 @JustinGainor @JackWestMD @christine_lovly @IbiayiMD @Latinamd @Joshua_Reuss @JuliaRotow @ReckampK @AngelQinMD @DocSacher @gadgeel @Annals_Oncology @ConorSteuerMD @BrunaPellini @LeXiuning @LaurenByersMD @DrSteveMartin @ZPiotrowskaMD @KCArbourMD @ValsamoA @maryjofidlerMD @Jia_Luo @collin_blakely @BeccaHeistMD @NEJM @JCO_ASCO #PostTest Q1️⃣ #TumorBoardTuesday
👉🏽#CME Eval 🔗 integrityce.com/tbtEval
🤔@LeciaSequist taught us ALK+ #NSCLC to kick off #LCAM, test your 🧠 with 3 quick Q’s❓
🧐Which 1L therapy would you pick for a 42yo male with LN+, ALK+, PD-L1- (CPS=0) NSCLC & multi bony metastases?
👉🏽#CME Eval 🔗 integrityce.com/tbtEval
🤔@LeciaSequist taught us ALK+ #NSCLC to kick off #LCAM, test your 🧠 with 3 quick Q’s❓
🧐Which 1L therapy would you pick for a 42yo male with LN+, ALK+, PD-L1- (CPS=0) NSCLC & multi bony metastases?
@TumorBoardTues @ALKLungCancer @EricBernicker @MurryWynes @JessicaJLinMD @StephenVLiu @n8pennell @HenningWillers @oncoOuLungCA @CharuAggarwalMD @MLadanyi @bensolomon1 @CoreyLangerMD @RamalingamMD @triparnasen @HwakeleeMD @JulieBrahmer @NarjustFlorezMD @HosseinBorghaei @benlevylungdoc @BrendonStilesMD @peters_solange @TonyMok9 @JustinGainor @JackWestMD @christine_lovly @IbiayiMD @Latinamd @Joshua_Reuss @JuliaRotow @ReckampK @AngelQinMD @DocSacher @gadgeel @Annals_Oncology @ConorSteuerMD @BrunaPellini @LeXiuning @LaurenByersMD @DrSteveMartin @ZPiotrowskaMD @KCArbourMD @ValsamoA @maryjofidlerMD @Jia_Luo @collin_blakely @BeccaHeistMD @NEJM @JCO_ASCO #PostTest Q2️⃣ #TumorBoardTuesday #NSCLC
👉🏽Free #CME🔗: integrityce.com/tbt
🧐Which testing methodology is the 🥇 gold standard for detecting ALK rearrangements?
👉🏽Free #CME🔗: integrityce.com/tbt
🧐Which testing methodology is the 🥇 gold standard for detecting ALK rearrangements?
@TumorBoardTues @ALKLungCancer @EricBernicker @MurryWynes @JessicaJLinMD @StephenVLiu @n8pennell @HenningWillers @oncoOuLungCA @CharuAggarwalMD @MLadanyi @bensolomon1 @CoreyLangerMD @RamalingamMD @triparnasen @HwakeleeMD @JulieBrahmer @NarjustFlorezMD @HosseinBorghaei @benlevylungdoc @BrendonStilesMD @peters_solange @TonyMok9 @JustinGainor @JackWestMD @christine_lovly @IbiayiMD @Latinamd @Joshua_Reuss @JuliaRotow @ReckampK @AngelQinMD @DocSacher @gadgeel @Annals_Oncology @ConorSteuerMD @BrunaPellini @LeXiuning @LaurenByersMD @DrSteveMartin @ZPiotrowskaMD @KCArbourMD @ValsamoA @maryjofidlerMD @Jia_Luo @collin_blakely @BeccaHeistMD @NEJM @JCO_ASCO #PostTest Q3️⃣ #TumorBoardTuesday
👉🏽 #CME Eval 🔗 integrityce.com/tbtEval
👉🏽 ALL CME🔗: integrityce.com/tbt
🧐 Which first-line therapy would you select for a 42-year-old male with ALK+ #NSCLC and metastases to the brain?
👉🏽 #CME Eval 🔗 integrityce.com/tbtEval
👉🏽 ALL CME🔗: integrityce.com/tbt
🧐 Which first-line therapy would you select for a 42-year-old male with ALK+ #NSCLC and metastases to the brain?
• • •
Missing some Tweet in this thread? You can try to
force a refresh



