
2/The Effect of COVID on Clinical Research by Drs. Laughlin and Evans:
—Significant increase in new onset diabetes
—A lot of COVID specific research for years to come
—COVID19 disproportionately impacted female scientists, parents and caregivers #OW2022
—Significant increase in new onset diabetes
—A lot of COVID specific research for years to come
—COVID19 disproportionately impacted female scientists, parents and caregivers #OW2022



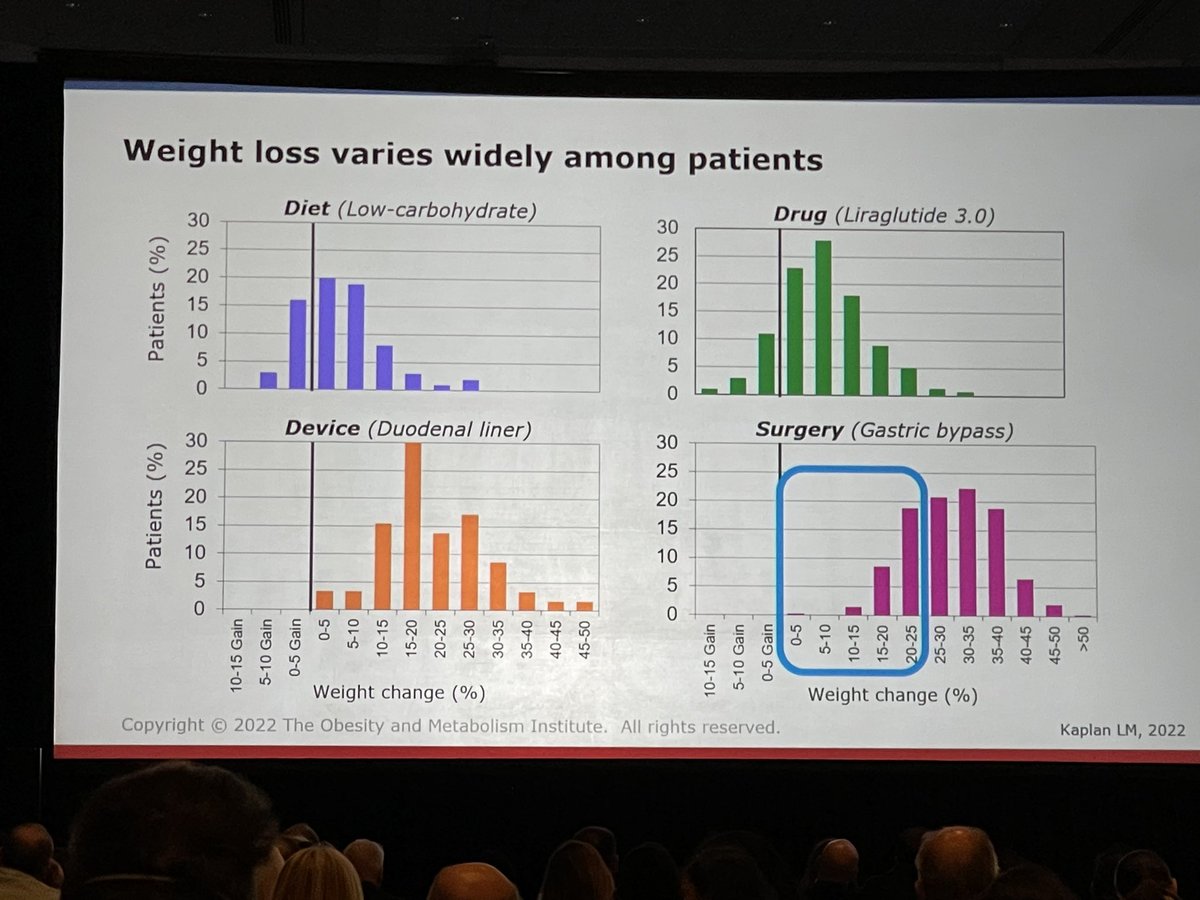
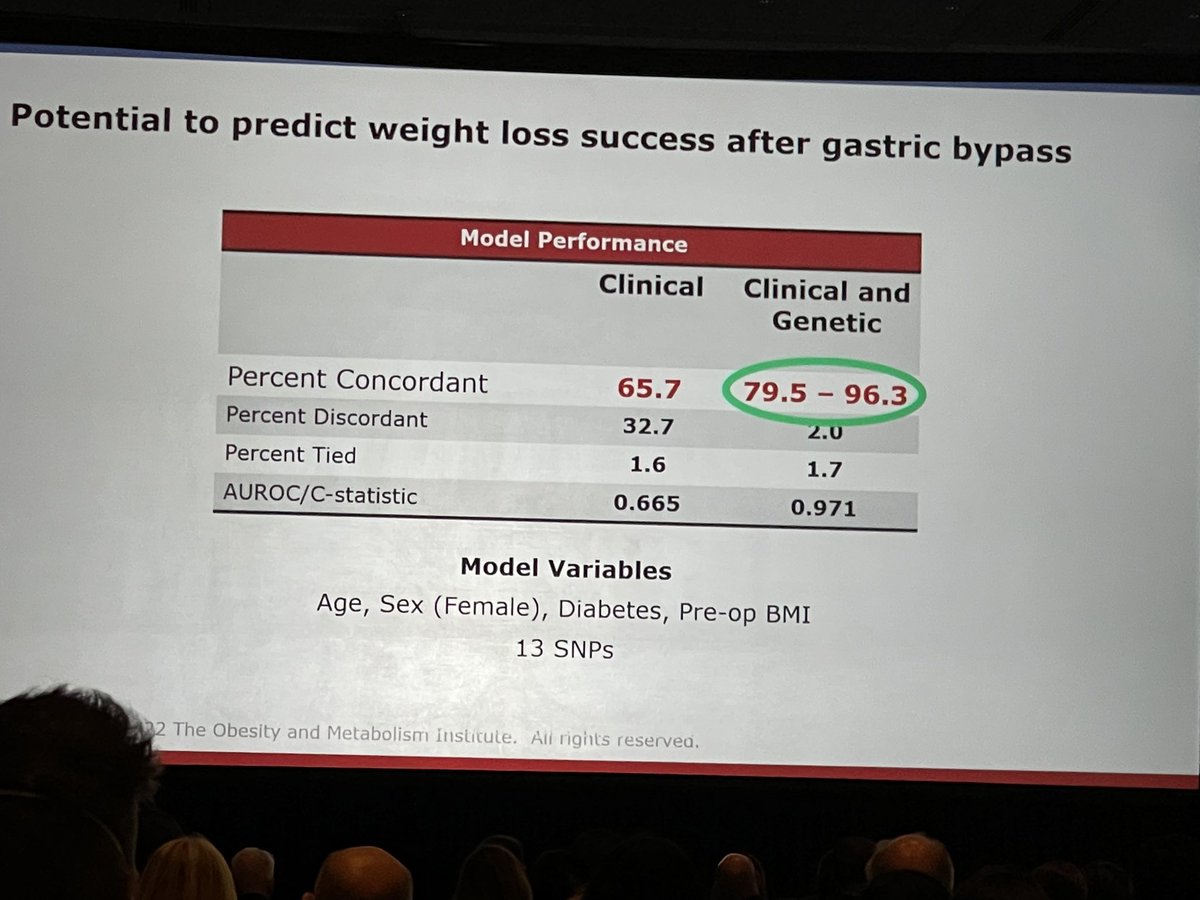
3/Update on the Use of Genetic Information to Tailor Obesity Treatment by Dr. Kaplan:
—People respond uniquely to treatments
—Genetic info can be used to predict treatment response and risk for weight gain over one’s life
—Precision genetic research IS EARLY #OW2022
—People respond uniquely to treatments
—Genetic info can be used to predict treatment response and risk for weight gain over one’s life
—Precision genetic research IS EARLY #OW2022


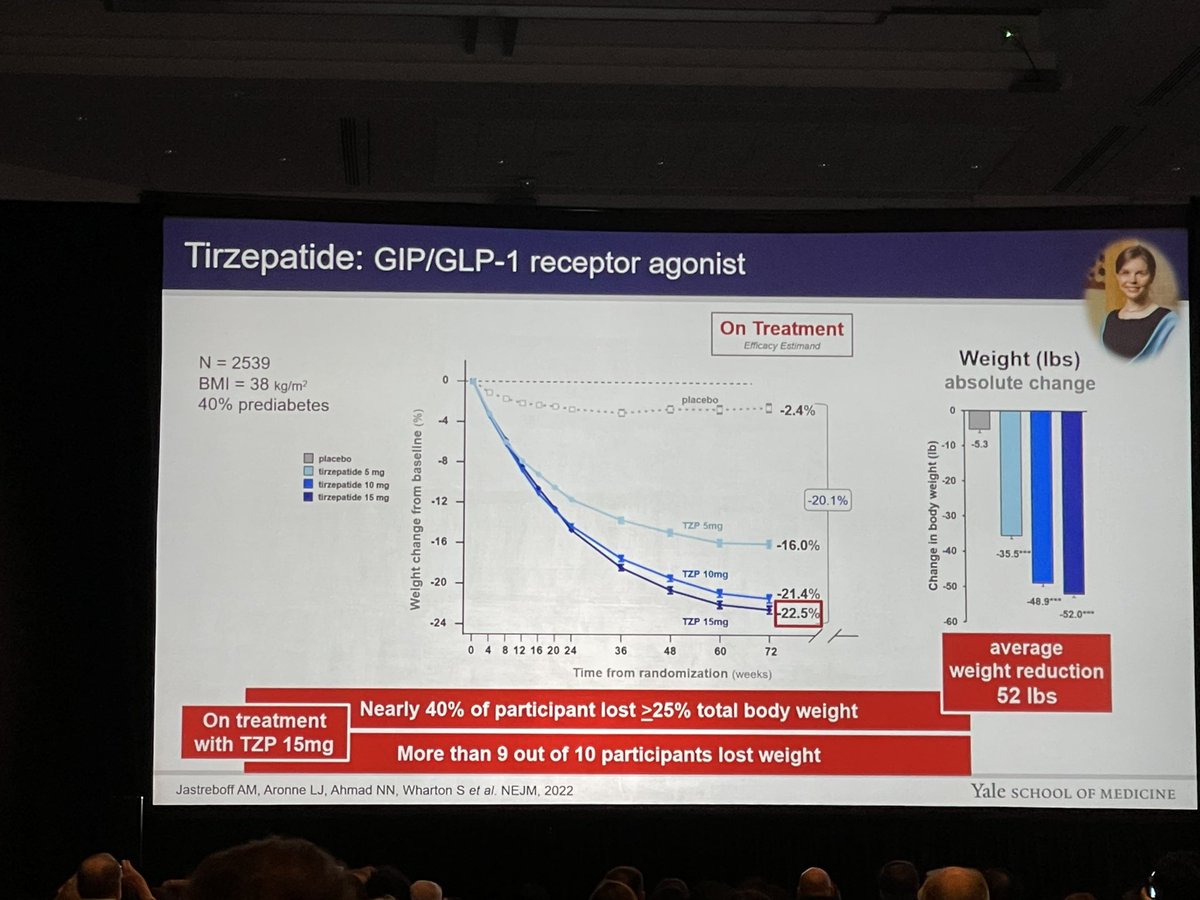
4/New Developments in Anti-Obesity Pharmacotherapy by @AniaJastreboff:
—We are entering a new era of obesity treatments
—Nutrient-stimulated hormone (NuSH)-based therapies will revolutionize obesity treatment and MEDICINE
**credit to Ania for NuSH. She owns it. 😂 #OW2022
—We are entering a new era of obesity treatments
—Nutrient-stimulated hormone (NuSH)-based therapies will revolutionize obesity treatment and MEDICINE
**credit to Ania for NuSH. She owns it. 😂 #OW2022


5/ GIP/GLP1-RA changed the game!
- -
>95% lost a clinically significant amount of weight at 15 mg dose!!!🤯
**many more exciting studies investigating the health benefits of this combo! #OW2022
- -
>95% lost a clinically significant amount of weight at 15 mg dose!!!🤯
**many more exciting studies investigating the health benefits of this combo! #OW2022



7/The future of NuSH-based therapies is bright! An incredible number of NuSH-based molecules in development!!! #OW2022




8/Novel therapeutics treat OBESITY!
- -
They are not weight loss drugs. They treat the underlying pathophysiology‼️ It’s time to move beyond weight-centric conversations and start talking about disease treatment and health benefits! 👏🏻👏🏻#OW2022
- -
They are not weight loss drugs. They treat the underlying pathophysiology‼️ It’s time to move beyond weight-centric conversations and start talking about disease treatment and health benefits! 👏🏻👏🏻#OW2022


9/Reducing Barriers to Treatment: Insurance Coverage by @ConscienHealth:
We’ve created a broken system of care for obesity founded on scientific ignorance and structural racism. #OW2022
We’ve created a broken system of care for obesity founded on scientific ignorance and structural racism. #OW2022
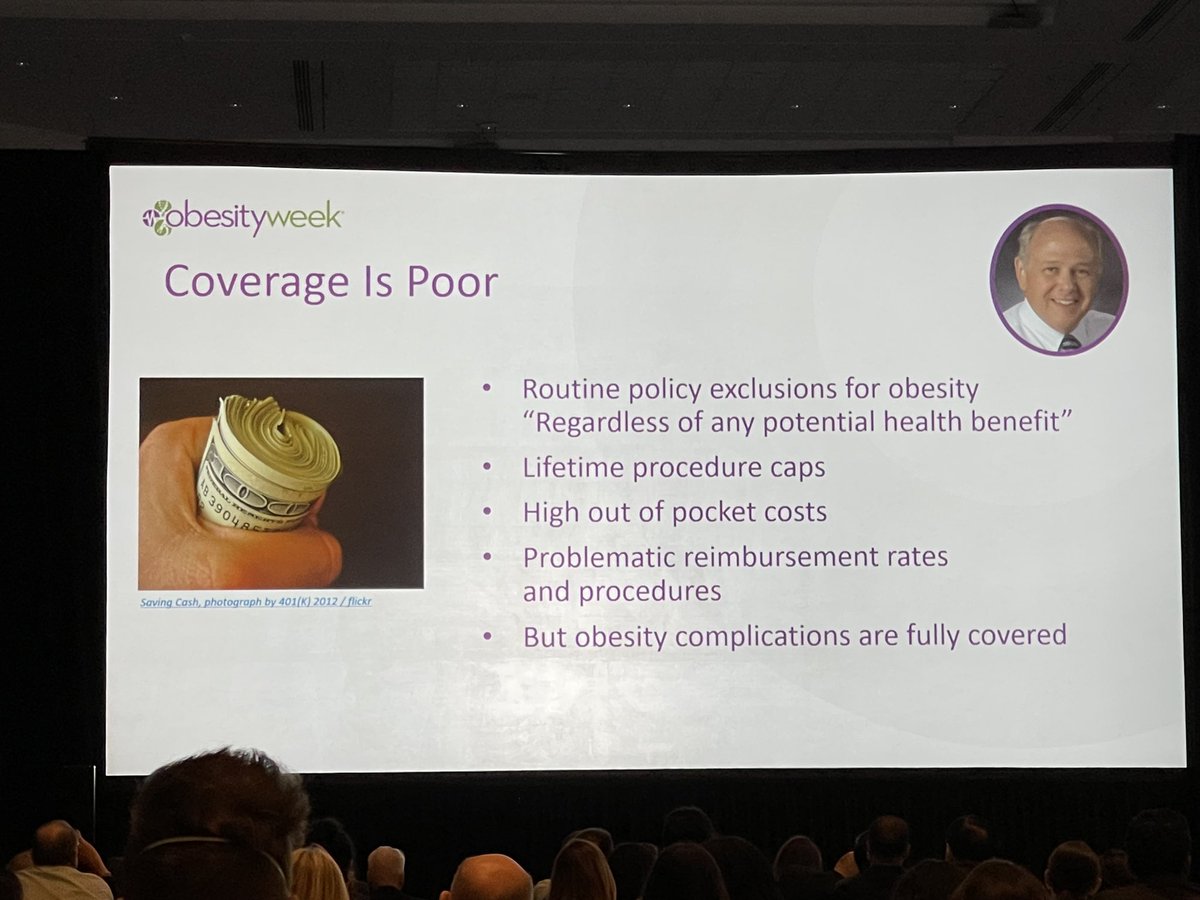


10/Biases rationalized care denial…FORTUNATELY, things are changing!! People are noticing and policies are changing. #OW2022




11/Metabolically Healthy Obesity by Dr Klein:
—Metabolically healthy obesity exists
—With strict criteria, it likely represents 7-13% of PwO
—Adiposity-related complications associated with insulin pathophysiology #OW2022
—Metabolically healthy obesity exists
—With strict criteria, it likely represents 7-13% of PwO
—Adiposity-related complications associated with insulin pathophysiology #OW2022




12/Questioning dogma related to obesity complications:
—Adipose expansion or spillover hypothesis is not supported
—Adipocyte size dysfunction hypothesis is not supported
—Inflammatory hypothesis is not supported
👉🏻IS IT ALL ABOUT INSULIN? 🧐🤔 #OW2022
—Adipose expansion or spillover hypothesis is not supported
—Adipocyte size dysfunction hypothesis is not supported
—Inflammatory hypothesis is not supported
👉🏻IS IT ALL ABOUT INSULIN? 🧐🤔 #OW2022


• • •
Missing some Tweet in this thread? You can try to
force a refresh















