#Stitch Puncture .
#Definition.
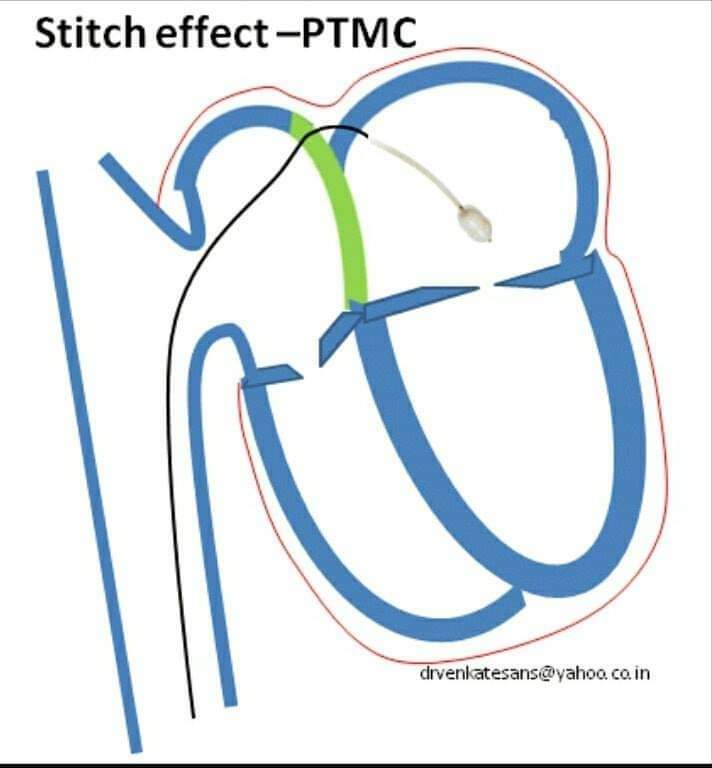
Stitch effect is a rare complication where the needle pierces the intrapericardial space from the right atrial side and re-enter the left atria
#Definition.
Stitch effect is a rare complication where the needle pierces the intrapericardial space from the right atrial side and re-enter the left atria
#Mechanism.
•Alignment of IAS with reference to RA and LA is key a determinant
•Normally RA & LA Roofs lie in same plane & IAS makes their common wall
•In MS LA can outgrow RA , bringing superior aspect of LA in a different plane with reference to IAS
•Alignment of IAS with reference to RA and LA is key a determinant
•Normally RA & LA Roofs lie in same plane & IAS makes their common wall
•In MS LA can outgrow RA , bringing superior aspect of LA in a different plane with reference to IAS
•The IAS puncture site may overshoot , enter the pericardial space and stitches the non IAS aspect of RA and LA together ,
& Entry into LA occurs through a false pericardial track
& Entry into LA occurs through a false pericardial track
#Different Stitch Routes can occur
1.IAS-Pericardial space -LA roof
2.RA-Pericardial space -LA roof
3.RA-Pericardial space -Extra cardiac-Reenter LA
1.IAS-Pericardial space -LA roof
2.RA-Pericardial space -LA roof
3.RA-Pericardial space -Extra cardiac-Reenter LA
#Possible Bleeding Points;
There can be two sites of active bleeding .One from RA exit point and other from LA entry point of needle.Extra-cardiac oozing can also occur if the needle has pierced the outer pericardium before entering LA.
There can be two sites of active bleeding .One from RA exit point and other from LA entry point of needle.Extra-cardiac oozing can also occur if the needle has pierced the outer pericardium before entering LA.
#When to Suspect.
If, after advancement of the catheter/needle, there is no recording of LA pressure, then there may have been perforation of the atrial wall.
#Management;
1.Urgent Shifting to Cardiac Surgery
2.Pericardiocentesis may be needed if Cardiac Temponade.
If, after advancement of the catheter/needle, there is no recording of LA pressure, then there may have been perforation of the atrial wall.
#Management;
1.Urgent Shifting to Cardiac Surgery
2.Pericardiocentesis may be needed if Cardiac Temponade.
Guidelines
1 If only needle has perforated, it can be withdrawn safely (a situation similar to early pretransseptal techniques),
2 if much larger catheter has perforated, then major bleeding is inevitable and Pt should be sent for catheter removal at open thoracic surg.
1 If only needle has perforated, it can be withdrawn safely (a situation similar to early pretransseptal techniques),
2 if much larger catheter has perforated, then major bleeding is inevitable and Pt should be sent for catheter removal at open thoracic surg.
Note.
To differentiate those two circumstances, a tiny amount (0.1-0.3 ml) of contrast can be injected through the needle. If this causes staining outside the atrial cavity, then needle perforation is confirmed. .
To differentiate those two circumstances, a tiny amount (0.1-0.3 ml) of contrast can be injected through the needle. If this causes staining outside the atrial cavity, then needle perforation is confirmed. .
Needle can then be withdrawn to just within catheter tip while catheter remains absolutely static. A further injection of contrast is given via needle. If contrast swirls within atrial cavity, catheter has not exited the heart and can be withdrawn.
If further staining is seen, the patient requires surgery for safe catheter removal
@PCRonline
@TCTMD
@APSIC6
@GisGulf
@mmamas1973
@mirvatalasnag
@PCRonline
@TCTMD
@APSIC6
@GisGulf
@mmamas1973
@mirvatalasnag
• • •
Missing some Tweet in this thread? You can try to
force a refresh