Florida's Boards of Medicine & Osteopathic Medicine voted to no longer allow new medical gender transitions in <18 in general medical settings (but allowed minors already in treatment to proceed with hormones). Poor quality of evidence was the stated basis for the new ban. /1
America’s medical societies insist that evidence proves the safety & efficacy of youth gender transition. European medical authorities, and now Florida’s Boards of medicine state the evidence of benefits is highly unreliable and the risks are real. How does one reconcile this? /2
The answer lies in what one means by an "evidence review." There is a critical difference between a “systematic review of evidence”—the cornerstone of evidence-based medicine (relied on in Europe)—and a vague claim of "completed evidence reviews” by @aap_peds, @wpath & others. /3
A systematic review (SR) analyzes all the available studies that meet pre-specified criteria, and does so in a reproducible way. Another researcher, following the same methodology, should get the same result. Unlike SRs, “evidence reviews” can "cherry-pick" studies. /4
Another key difference is in what happens after the studies are identified. Systematic reviews don’t take study conclusions at “face value." They scrutinize study methods and its reliability. In contrast, "evidence reviews" can get away with simply restating study conclusions. /5
The evaluation of study methods and "risk of bias" (systematic error) follows a rigorous and reproducible process. For non-randomized studies, one of the best methods is known as ROBINS-I. One can think of it as "lie detector test" for studies. /6
methods.cochrane.org/methods-cochra…
methods.cochrane.org/methods-cochra…
Because problems in methodology can introduce a systematic error (bias) into the results, and render a study's conclusions not trustworthy, a "risk of bias" assessment is a key step in a “systematic review”—but not in a generic “evidence review.” /7
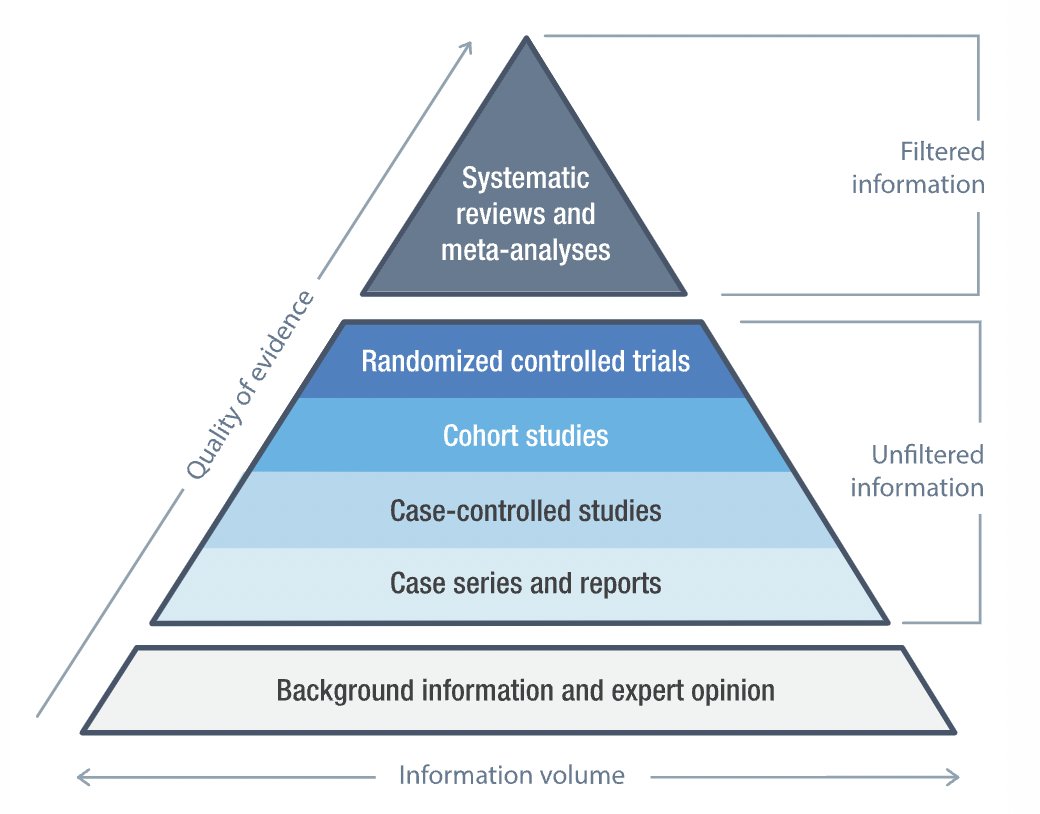
Systematic reviews (SR) state the research question; have clear study eligibility criteria; don't cherry-pick studies; & assess the quality of the evidence found. The conclusions synthesize the totality of the evidence. That's why SRs reside at the top of the evidence pyramid. /8 
Every systematic review (SR) in gender medicine has concluded that the evidence is of “very low/low” quality, and that the benefits reported by the studies are uncertain due to poor study designs. This is true even for the Endocrine Society's own SR. /9
cass.independent-review.uk/nice-evidence-…
cass.independent-review.uk/nice-evidence-…
It must be said that all the evidence is of low quality. Not only the benefits but also the risks. Thus, both the benefits and the risks of “gender-affirmation”—social transition, puberty blockers, cross sex hormones, and surgery—must be studied using rigorous study designs. /10
But one key risk is a matter of biological certainty. When puberty is blocked at the earliest stage (Tanner 2) & followed by cross-sex hormones (as recommended by the Endocrine Society)—infertility & likely sterility are assured. This is because eggs and sperm can't mature. /11
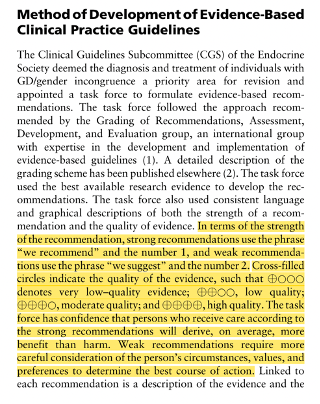
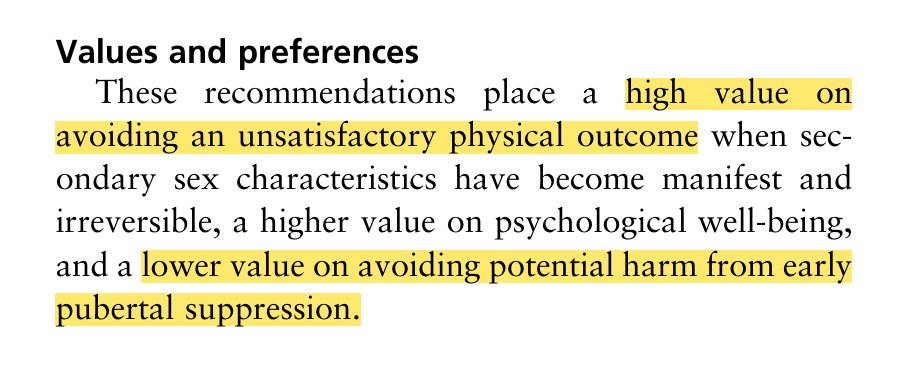
The Endocrine Society (ES) knows the evidence of benefits is of low quality. They also acknowledge the risk of harm. How do they justify their recommendations for hormonal treatments for minors? By placing a higher value on the desired sex appearance than on avoiding harm./12
Paradoxically, @WPATH claimed in SOC8 that a systematic review is not possible. This is demonstrably false. Several systematic reviews of evidence of youth gender transition have been conducted in Europe. WPATH itself commissioned a systematic review of evidence for its SOC8./13

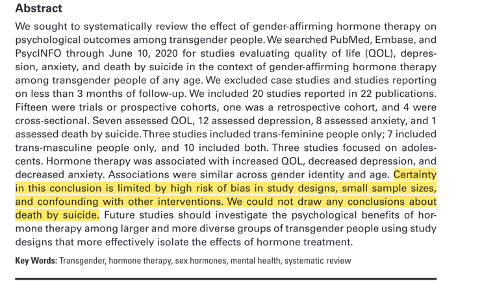
Although the systematic review (SR) funded by WPATH has many methodological problems (which the Journal of the Endocrine Society chose not to acknowledge), this SR came to a similar conclusion: the benefits reported by the studies are highly uncertain./14
academic.oup.com/jes/article/do…
academic.oup.com/jes/article/do…
Why Europe is hitting the breaks on pediatric gender transition is clear. The evidence for benefits is highly uncertain. The risks are real. Infertility & sterility are a biological certainty. A better question is, why are the U.S. medical societies going full-steam ahead? /end
• • •
Missing some Tweet in this thread? You can try to
force a refresh