Dr @ljlaffin presents the results of the #SPORT trial. Rosuva 5mg/d lowered LDL significantly more than 6 dietary supplements commonly used for cholesterol health. In fact no supplement lowered LDL-C more that placebo and garlic supplement actually raised LDL. #AHA22 @AHAScience 
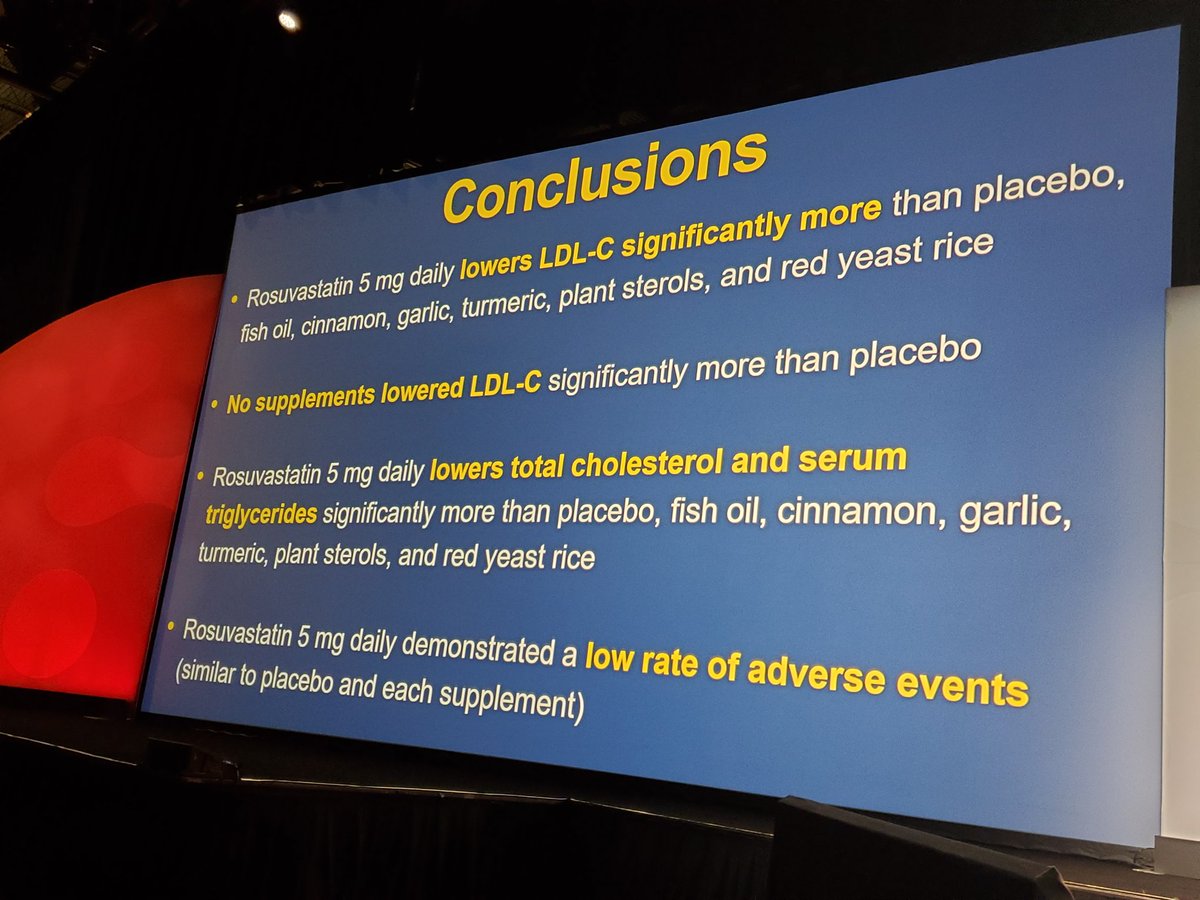


Notably in this short term trial, no increase in musculoskeletal or neurological symptoms or worsening glycemia with rosuva 5. All participants with rosuva 5 had LDL lowering (coin toss for supplements), 50% had LDL>40% reduced with rosuva 5. #AHA22




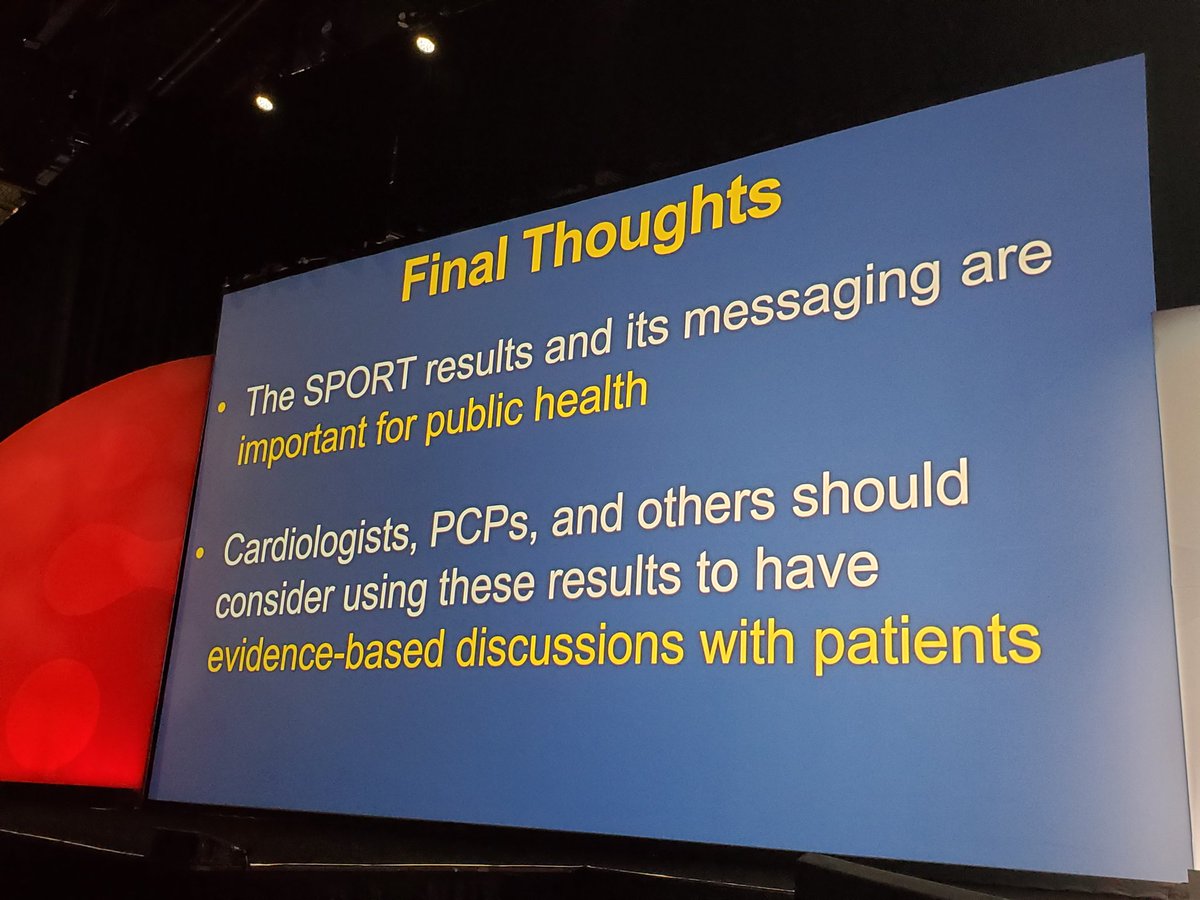
77% of US adults take supplements and $50 billion is spent annually in US on supplements. But do they lower LDL? These supplements advertise that they help heart health but no better in lowering LDL than placebo not even red yeast rice. @ljlaffin #AHA22 @AHAScience



• • •
Missing some Tweet in this thread? You can try to
force a refresh