01/ Buckle up, everyone, it’s time for a Tweetorial. Been working on this one for a while. This time, I’ll focus on the most common mesenchymal malignancy of the digestive tract: gastrointestinal stromal tumor (GIST). #pathology #gipath #PathTwitter
02/ GIST arises from the interstitial cells of Cajal. It can originate anywhere in the GI tract, though most cases occur in the stomach or small bowel. Rectum cases are uncommon, and GIST is very rare in the esophagus, colon, or appendix.
03/ Old terms for GIST include GANT (gastrointestinal autonomic nerve tumor) and leiomyoblastoma. These terms are no longer used, though you may run across them in older literature.
04/ Clinically, GISTs most often cause abdominal pain. They can also cause mucosal ulceration and hence bleeding. As I’ll mention later, sometimes they are encountered incidentally. Other times, they are widely metastatic at presentation.
05/ Grossly, GIST usually forms a round, well-circumscribed, fleshy mass. Intralesional hemorrhage may be prominent, especially in larger tumors. They can grow larger than 20 cm in some instances. 


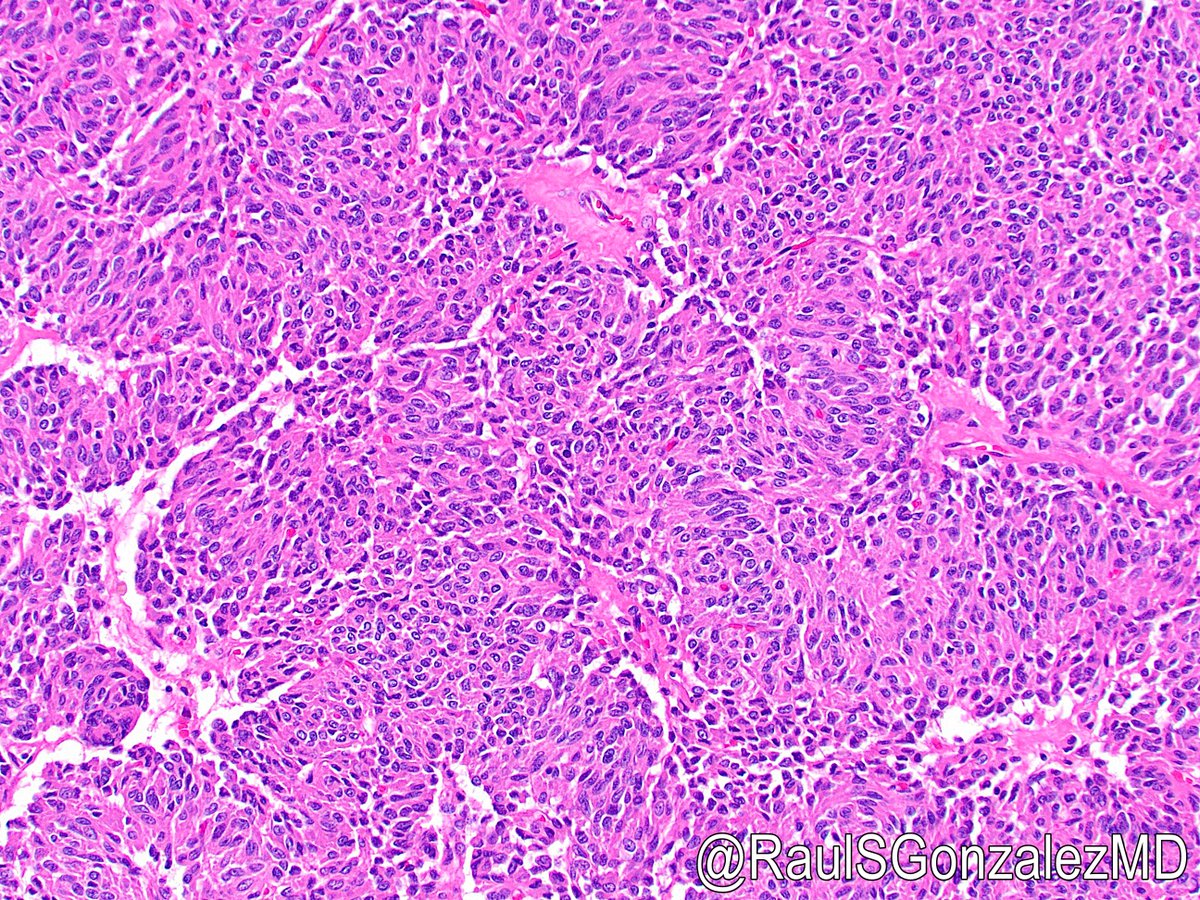
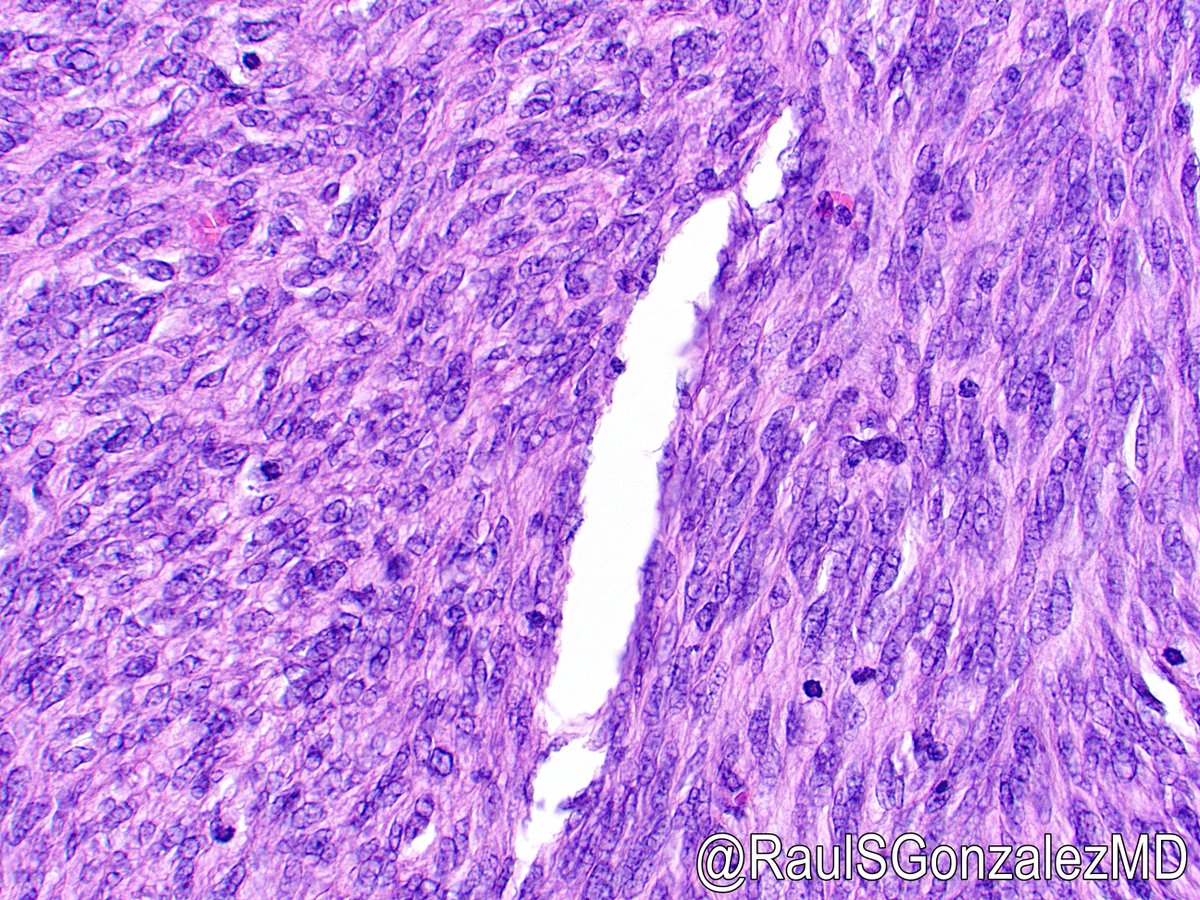
06/ GIST most commonly forms a spindle-cell lesion. Cells are arranged in fascicles and have slightly hyperchromatic nuclei with pointed ends. There are a few varieties of spindle-cell GIST, including one with prominent nuclear palisading.

07/ One interesting feature of spindle-cell GIST is paranuclear vacuoles, which are a helpful clue to the diagnosis. These are an artifact of formalin fixation and would not be seen on frozen section.

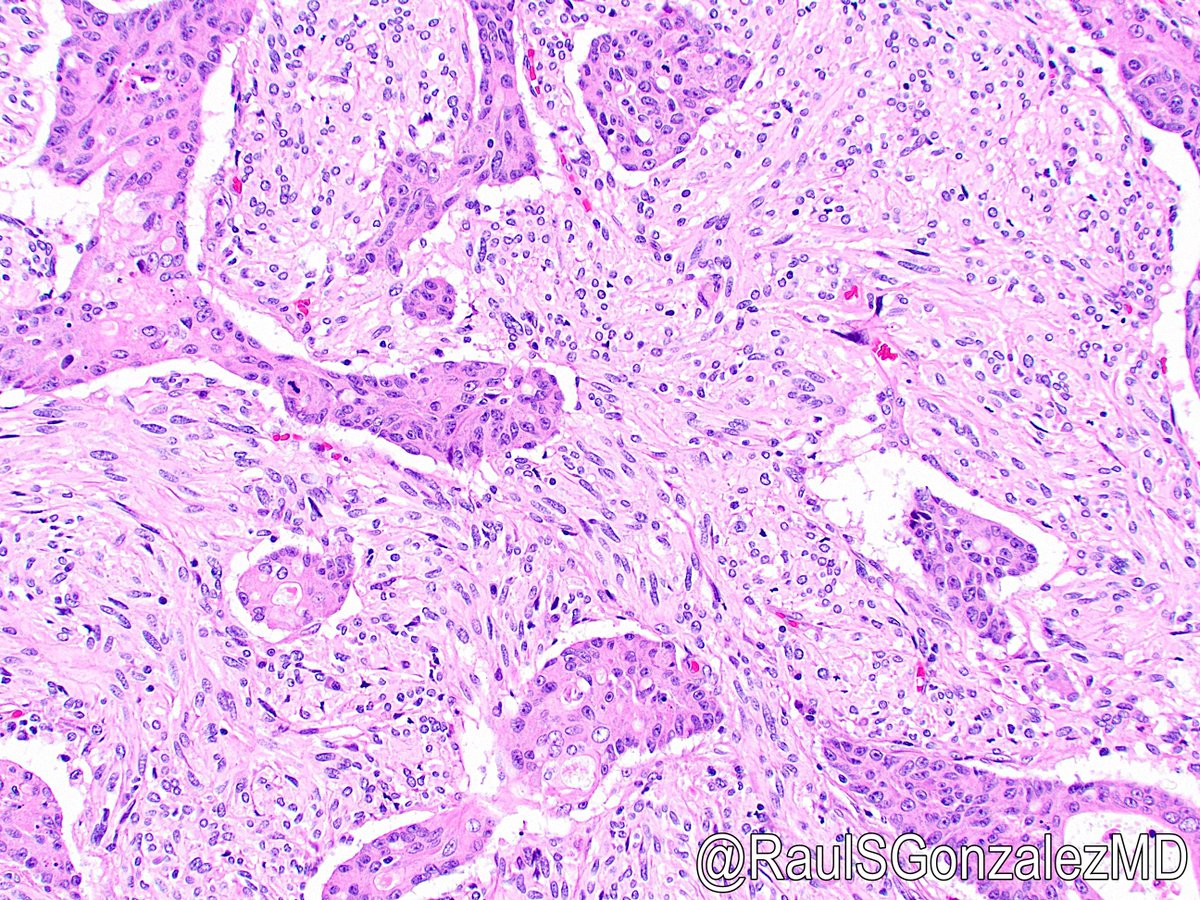
08/ GIST can also be epithelioid. These behave more aggressively overall and can have a wide range of appearances. Some cases also demonstrate both spindled and epithelioid areas.



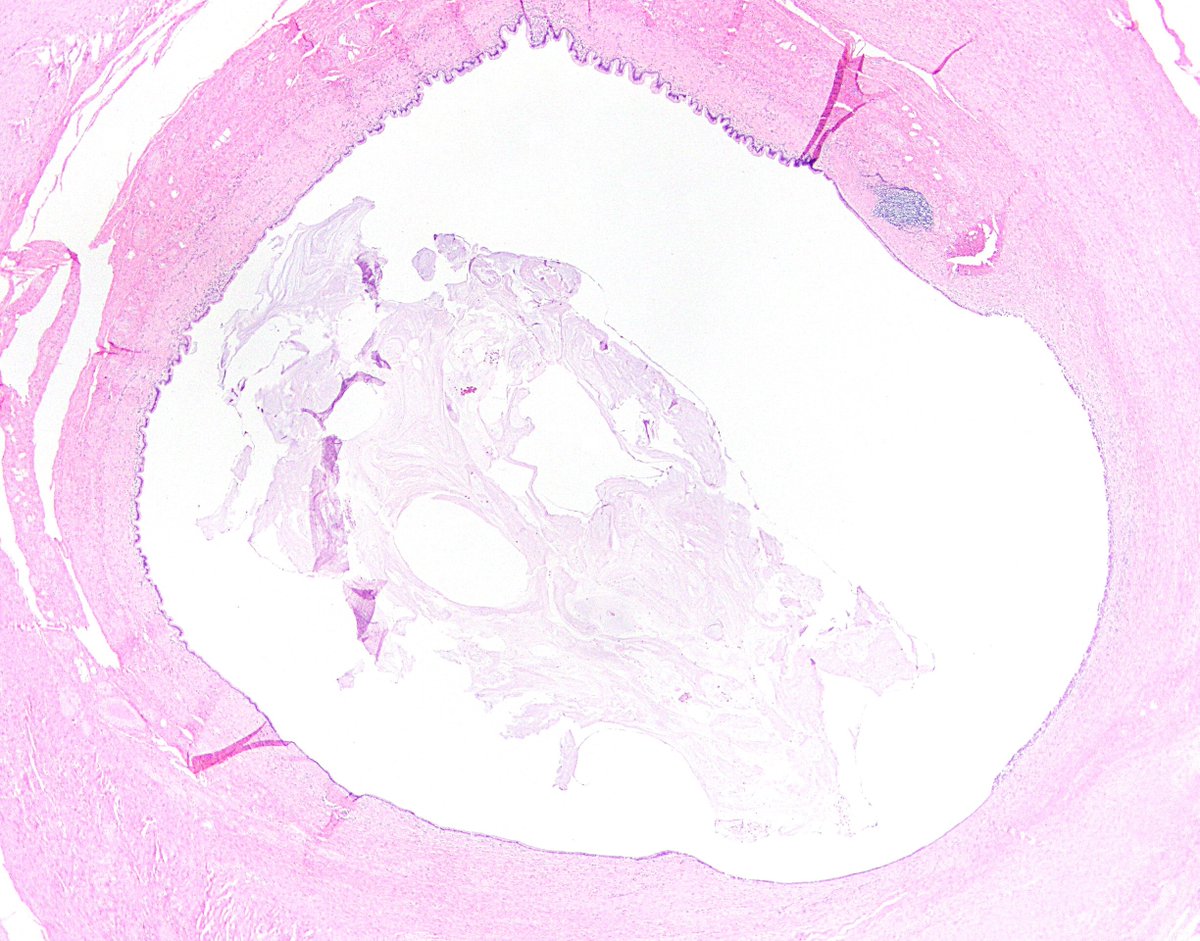
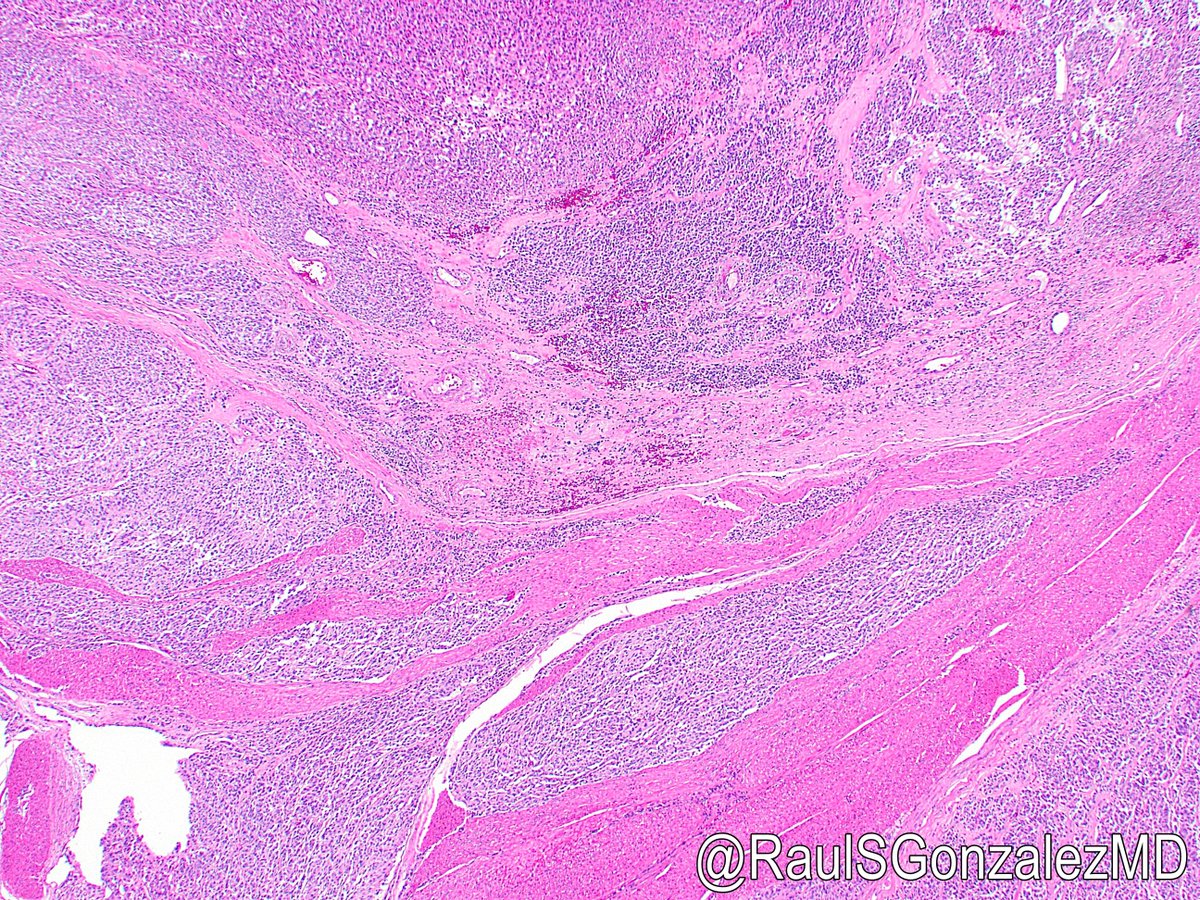
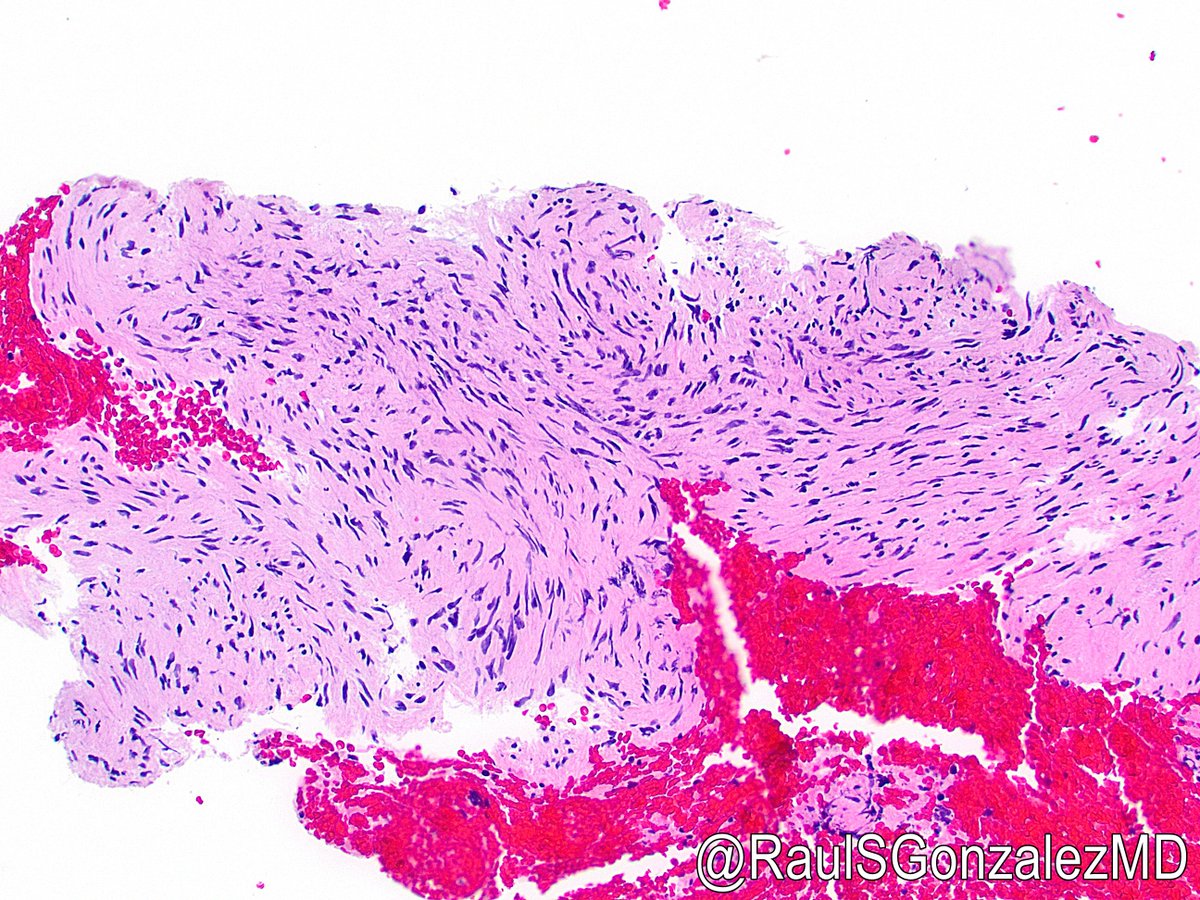
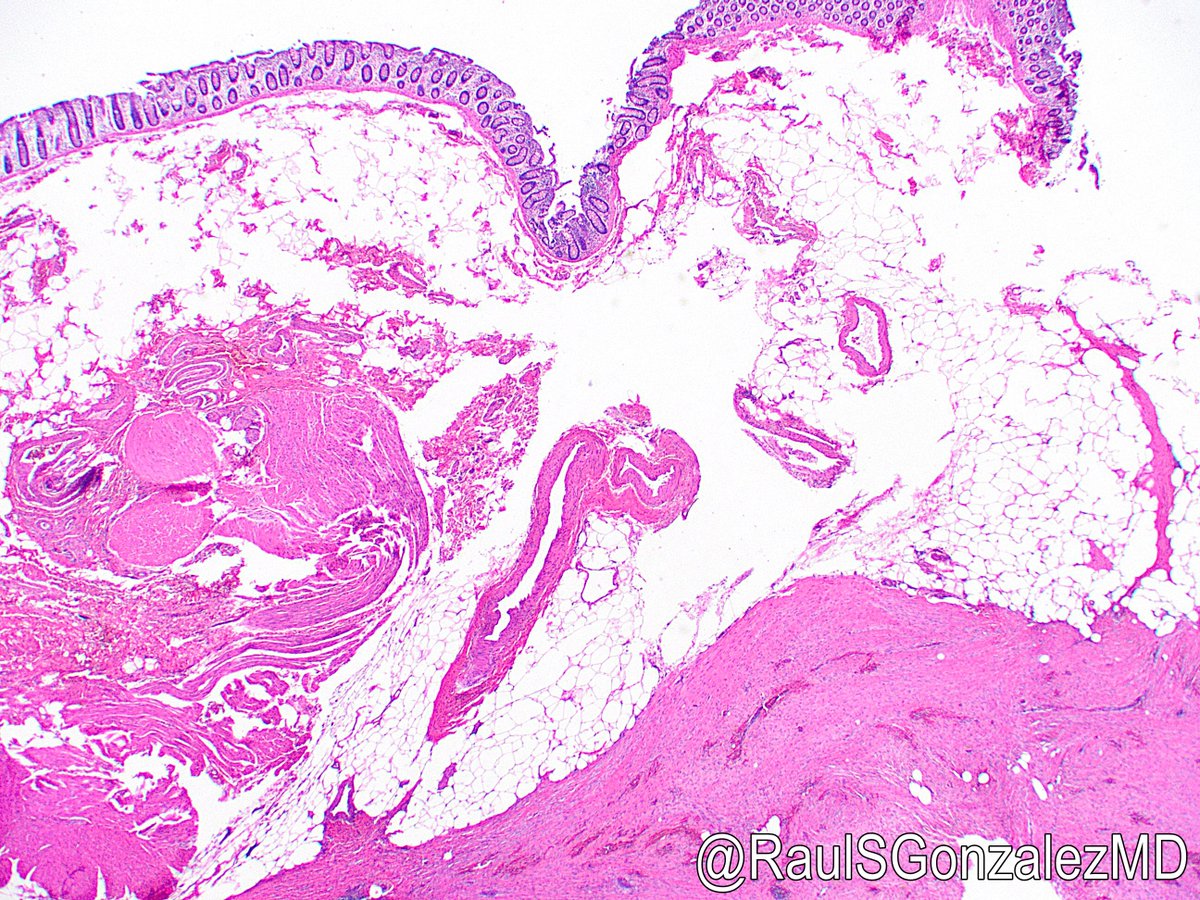
09/ GIST usually arise in the muscularis propria of the GI tract (see pic 1 and this great ref: bit.ly/3RZHvLc), though I’ve rarely seen them present endoscopically as a polyp (see pic 2).

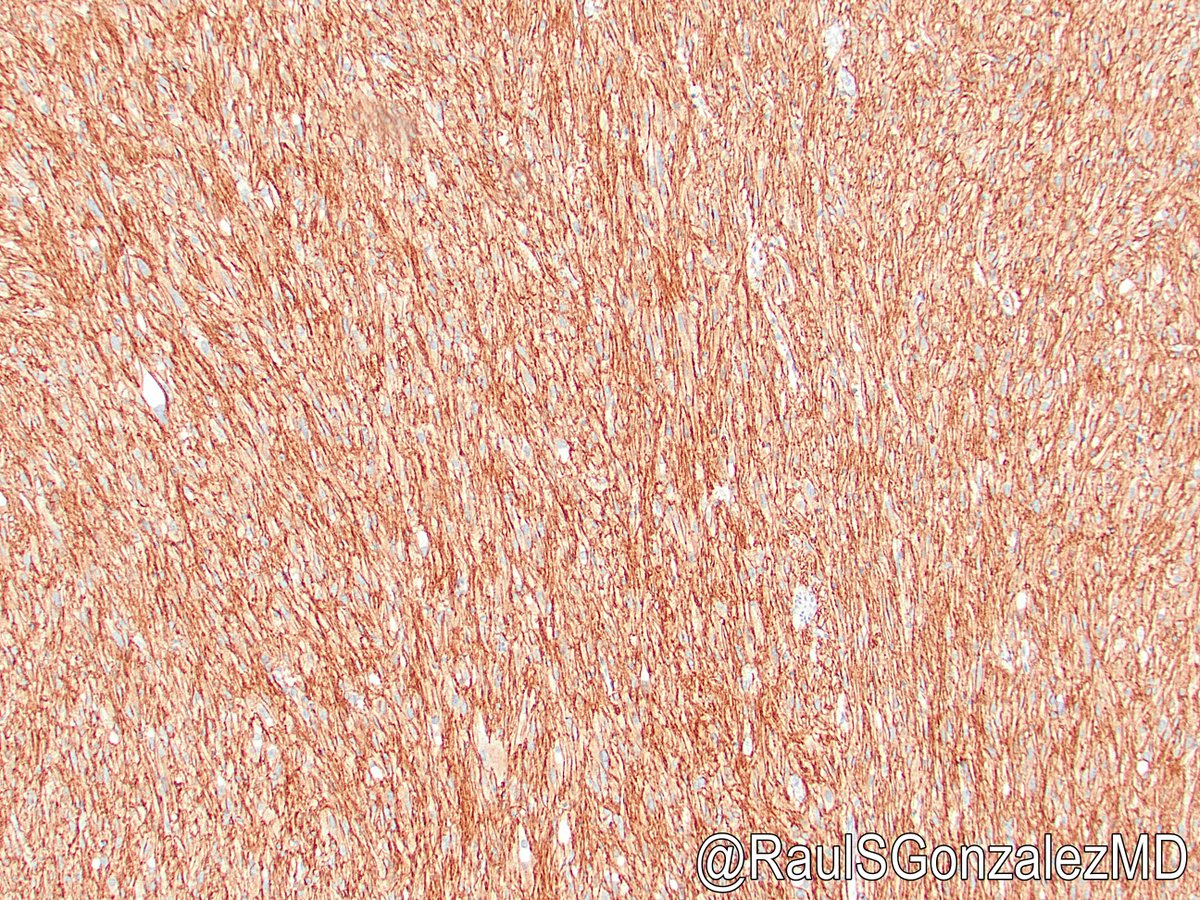
10/ The diagnosis of GIST can be confirmed using immunohistochemistry. The first marker used for this was CD34. This is of course nonspecific and not too helpful these days, as some mimics can also be positive for CD34 (as we’ll see).

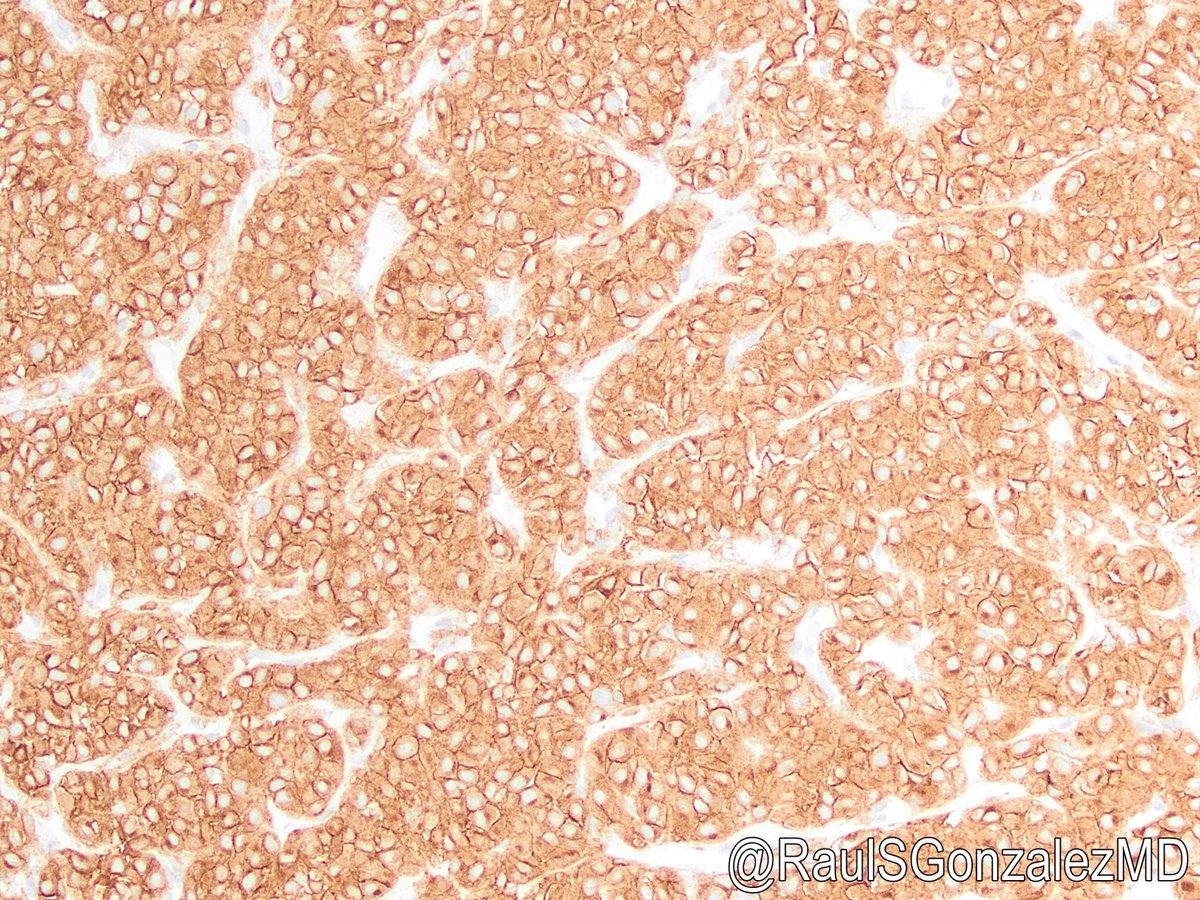
11/ More modern and more specific stains include CD117 (aka KIT -- calling it cKIT has fallen out of favor; pic 1) and DOG1 (Discovered On GIST 1; pic 2). There’s also the oft-overlooked protein kinase C theta.

12/ KIT and DOG1 are very helpful in diagnosing GIST. But do we need both KIT and DOG1 staining to make the diagnosis? I admit I still order both stains, since neither quite reaches 100% sensitivity. If one is positive, you’ve got a GIST.
13/ Once you’ve made the diagnosis of GIST, the next step is risk stratification. Not all GISTs behave aggressively, though certain features indicate a higher likelihood of metastasis or disease-related death.
14/ Several schemes have been proposed, but the AFIP criteria have arguably won out for pathologists. This estimates risk of progression (metastasis or tumor-related death) using tumor site, size, and mitotic rate (table from capatholo.gy/3Bhwq28).

15/ That table estimates behavior for gastric, small bowel, and rectal GISTs. Curious about esophageal, colonic, or appendiceal GISTs? There’s a table for those in this recent paper: bit.ly/3zxqmS1 (free supplementary table shown).

16/ When you’re counting mitotic figures, keep in mind that the denominator is no longer “50 high-power fields” (which varies across microscopes). Instead, count per 5 square millimeters (about 21 HPF on my scope).
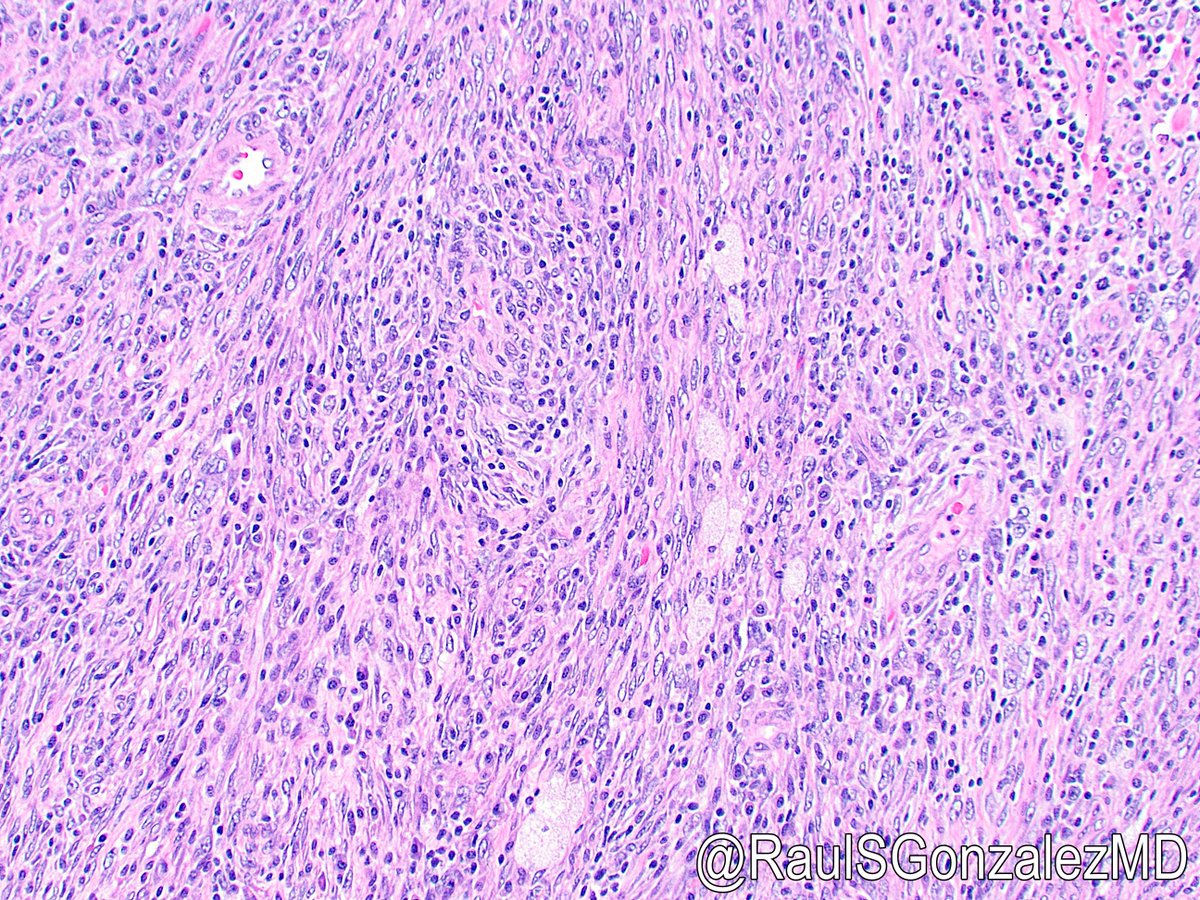
17/ It should go without saying, but always do the mitotic count! Don’t assume anything based on low-power appearance. This GIST looks on low power like it would be mitotically indolent, but high power tells a different story.

18/ Side note: You may remember some recent discussion on Twitter regarding how to distinguish true mitotic figures from mimics. Here are a few nice references: bit.ly/3zZHkbO and bit.ly/3zxEbPb
19/ Should we use PHH3 IHC to look for mitotic figures? I haven’t seen good literature on this, meaning it hasn’t been validated. Counts would almost certainly be higher than for H&E, which could throw off the risk stratification. So: no.
20/ While AFIP risk stratification is entrenched, other classification schemes continue to be suggested. One is the Nashville Risk Score, which uses size (7 cm), mitotic rate (>10 per 5 sq mm), and multifocality. Ref: bit.ly/3PRbBPg
21/ In addition to risk stratification, the AJCC also has staging criteria for GIST (see capatholo.gy/3Bhwq28). T-category staging uses tumor size (which we already know is a risk factor). N-category staging is binary, but ...

22/ GIST almost never metastasizes to lymph nodes! (Remember that “almost” for later.) In fact, if you have a resected GIST with no nodes in the specimen, the AJCC 8th edition book indicates you can call it pN0 because it’s so unlikely.
23/ Therapy for GIST (beyond surgery) focuses largely on tyrosine kinase inhibitors (TKIs), such as imatinib (Gleevec). This can be used for neoadjuvant or adjuvant treatment. TKI selection depends on tumor mutations, as we’ll discuss.
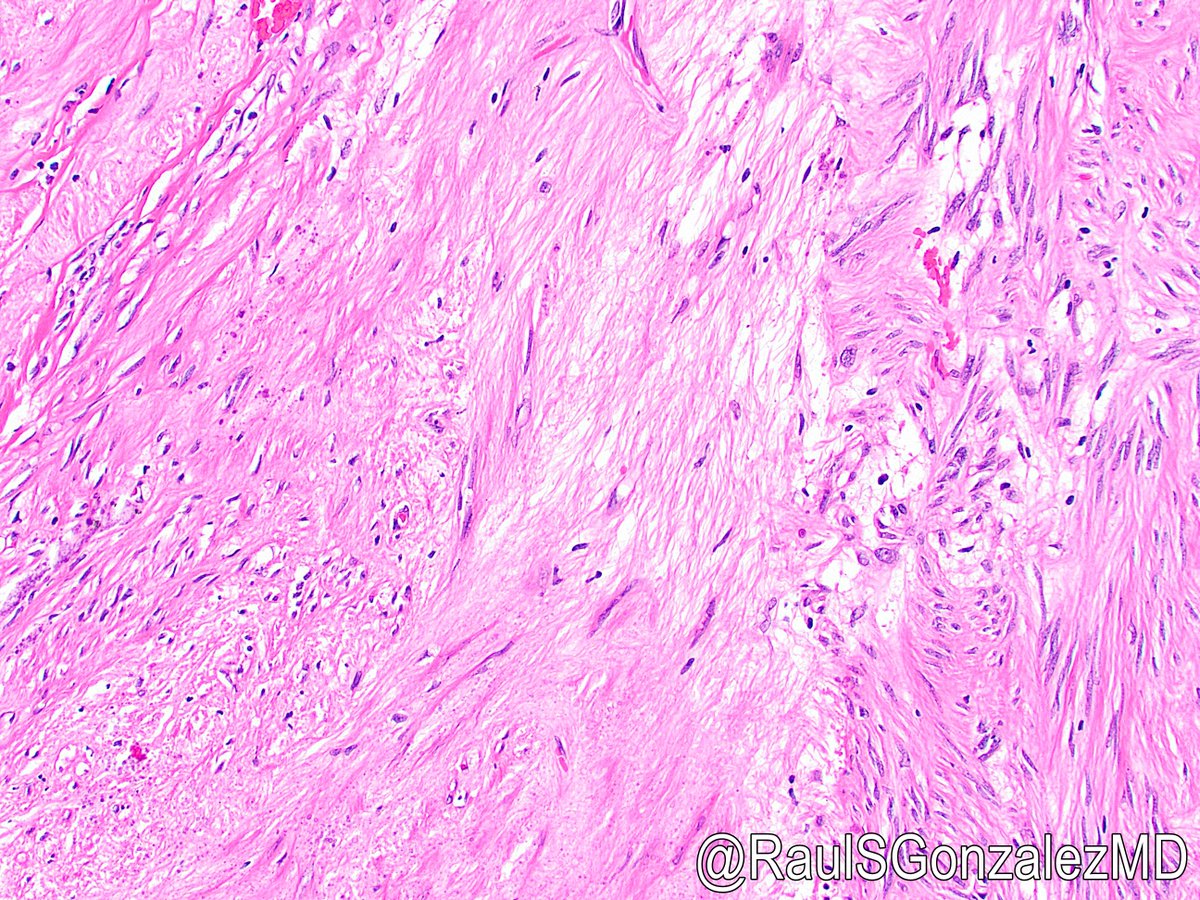
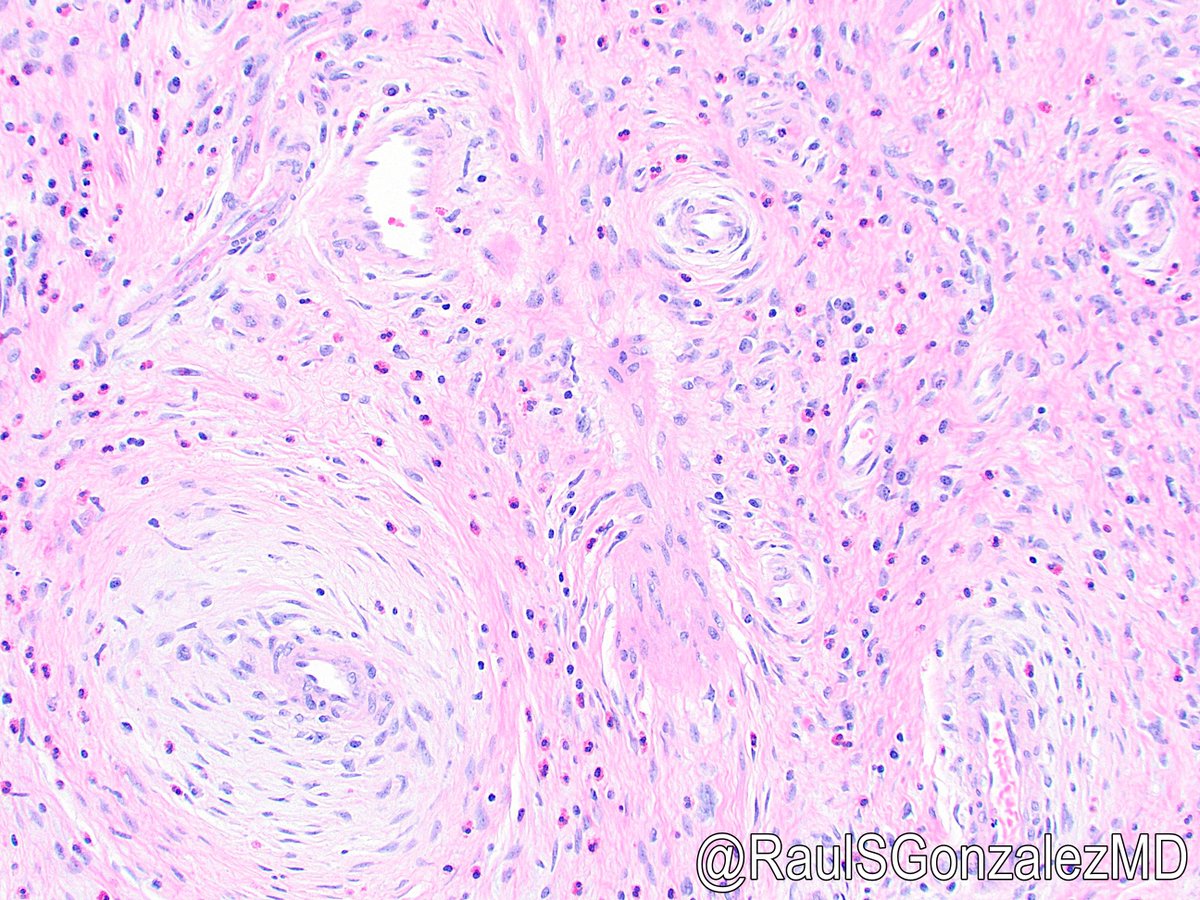
24/ Now for site-specific features. Gastric GISTs are common and usually spindled and low-risk. A few histologic patterns have been described, including paucicellular/sclerosing (pic 1) and palisading (pic 2). Ref: bit.ly/3vdhjTx
25/ Small bowel GISTs have a peculiar histologic finding: skeinoid fibers. These have unclear origin and significance but are usually seen in low-risk tumors.


26/ Appendiceal GISTs are almost always small and indolent, in addition to being quite rare. I’m only aware of one case report of a high-risk GIST in this location: bit.ly/3cItEcc

27/ GISTs of the esophagus (pic 1), colon, and rectum (pic 2) don’t have any striking individual characteristics. Most of them are composed of bland spindle cells.


28/ And finally, there’s the weird concept of extragastrointestinal stromal tumor, or EGIST. These are believed to originate in the GI tract but find their way into adjacent soft tissue sites, generally omentum, mesentery, or peritoneum.

29/ Wondering how a GIST becomes extra-gastrointestinal? They may just fall off! Check out this gross image of a gastric GIST just barely hanging on to the serosal surface by a thin strand of fibroconnective tissue.

30/ Now, let’s talk about the molecular features of GIST. There’s actually a lot to cover here (see pic, from bit.ly/3D6ul8Q), with relevance to IHC, prognosis, response to therapy, and even genetic syndromes. There’s even a CAP synoptic: capatholo.gy/3owMrdg

31/ The most commonly mutated gene in GIST is KIT (maybe 70-80% of cases). This is easy to remember, since most GISTs stain for KIT (CD117). Most of these mutations involve exon 11.
32/ However, GISTs with KIT exon 9 mutations require higher doses of imatinib. Plus, exon 13, 14, 17, and 18 mutations (usually secondary mutations) confer resistance to imatinib but not other TKIs.
33/ The next most commonly mutated gene is PDGFRA (10-15% of cases), usually but not always exon 18 D842V point mutations. This mutation also confers TKI resistance, but avapritinib targets the mutation and works well in those patients. These GISTs are still KIT-positive by IHC.
34/ Side note, there’s a PDGFRA immunostain that identifies GISTs with a mutation in that gene. Pic courtesy of Dr. David Papke. More info here: bit.ly/3Bl3juX
35/ The next molecular GIST subtype is very interesting. These have mutations in genes that encode for succinate dehydrogenase (SDH) subunit proteins, like SDHA, SDHB, SDHC, and SDHB. These were once called “wild-type” GISTs.
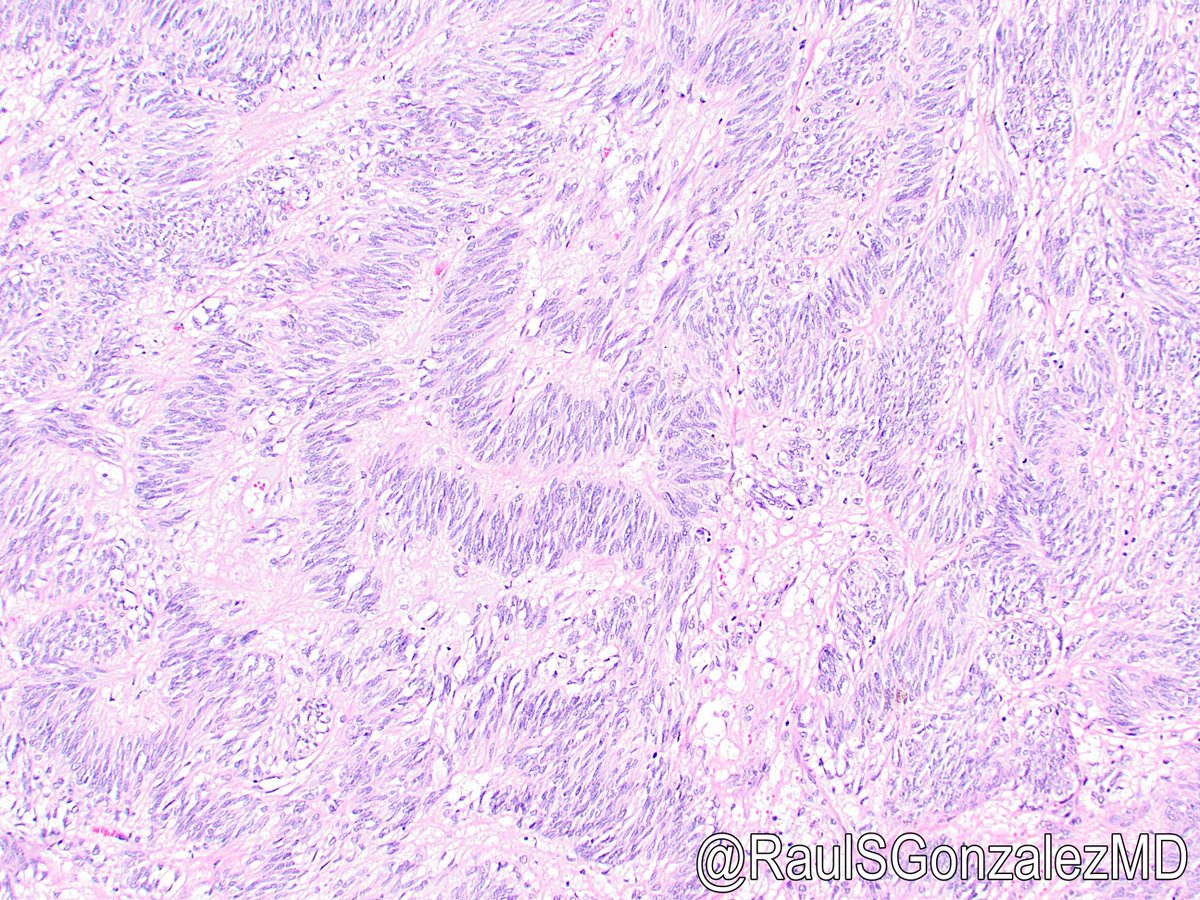
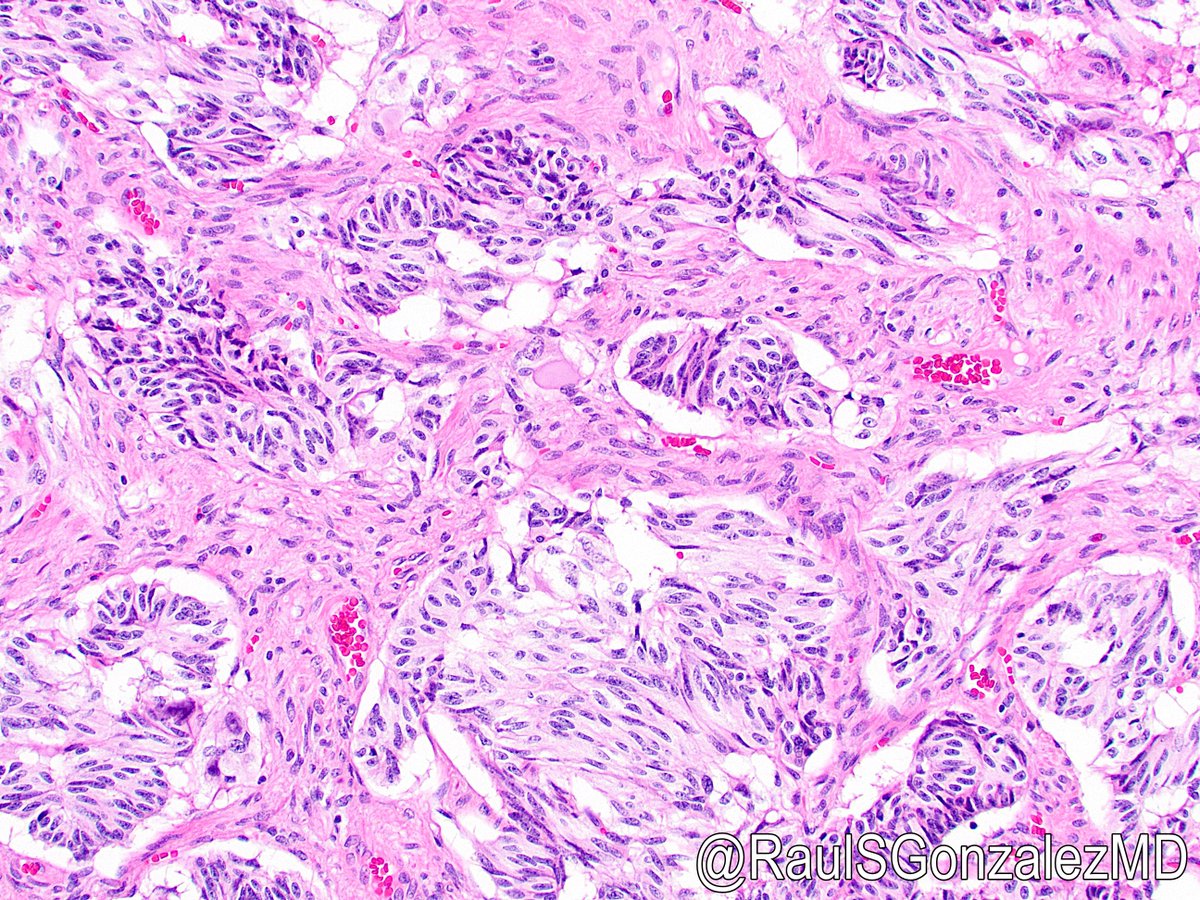
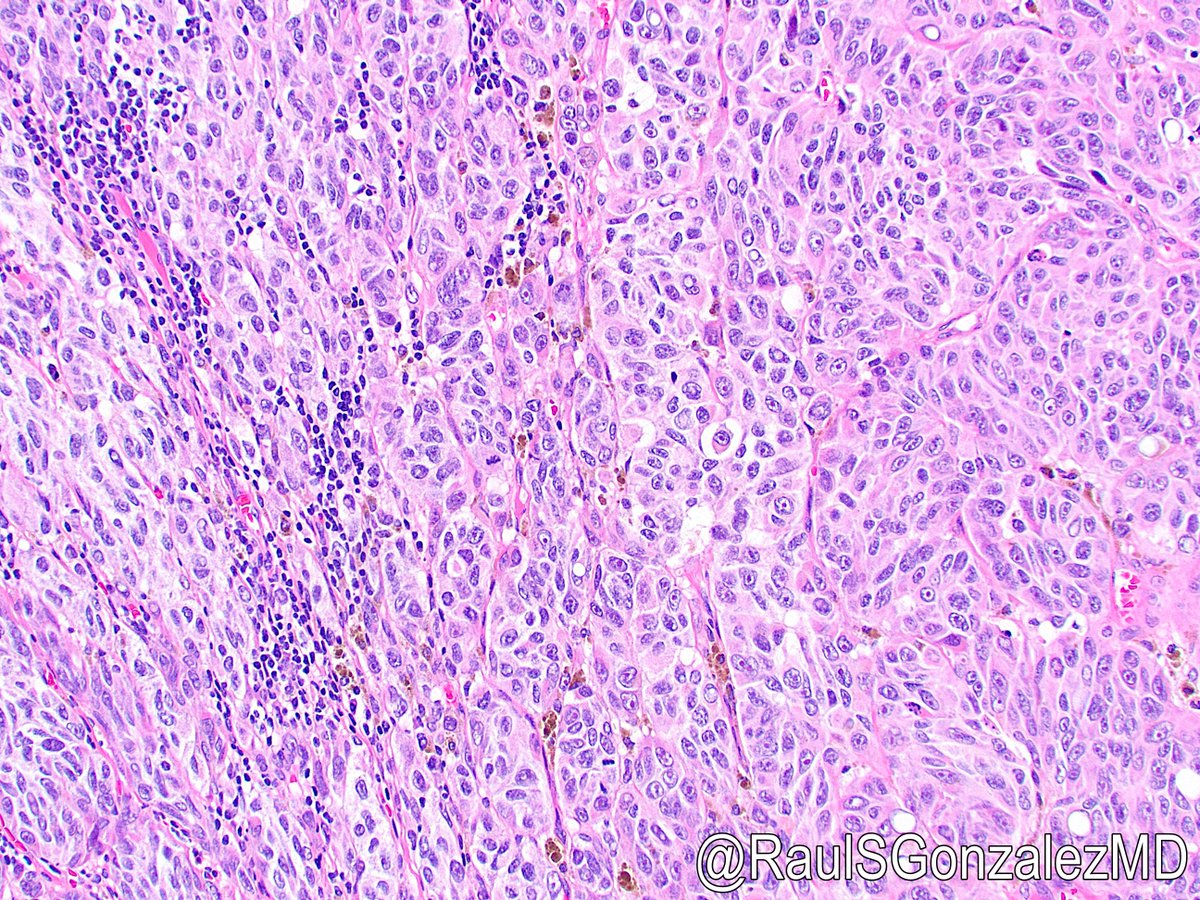
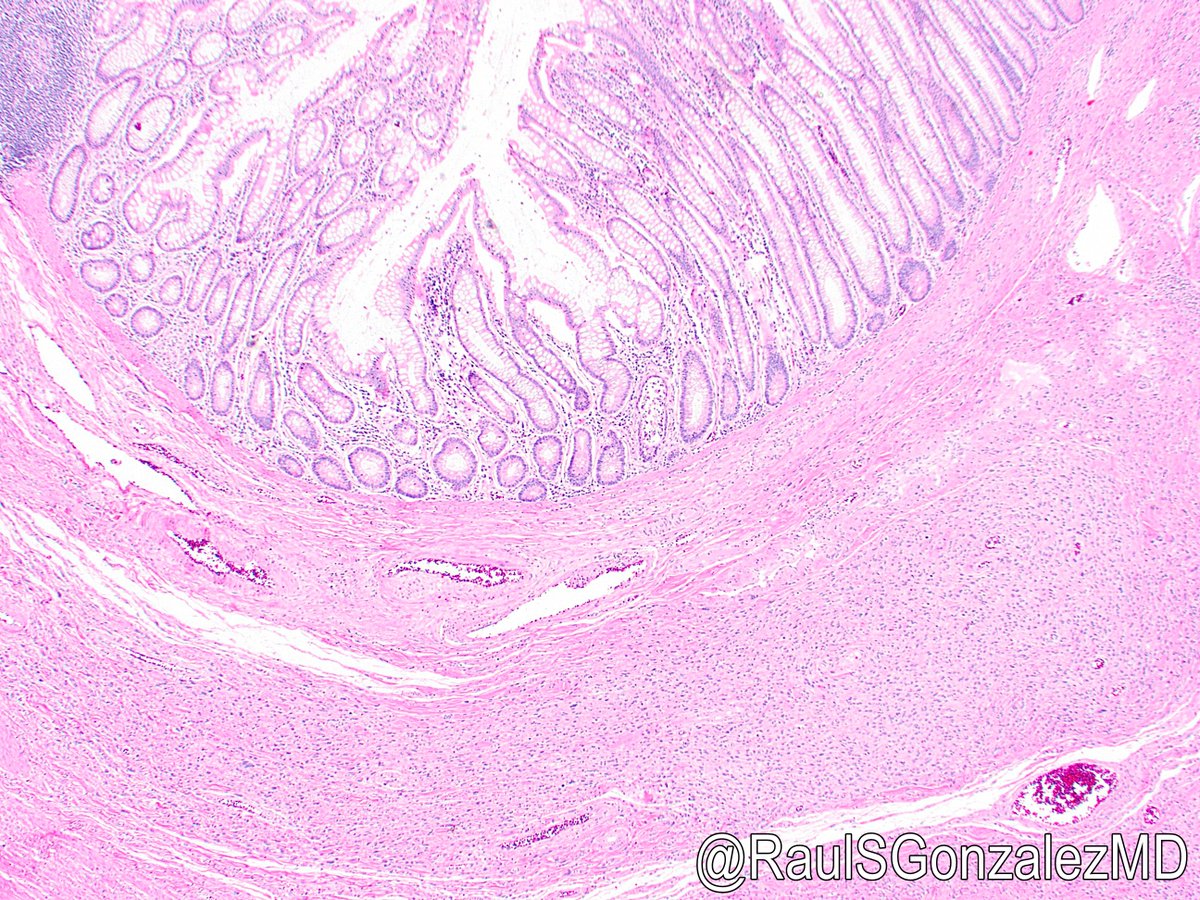
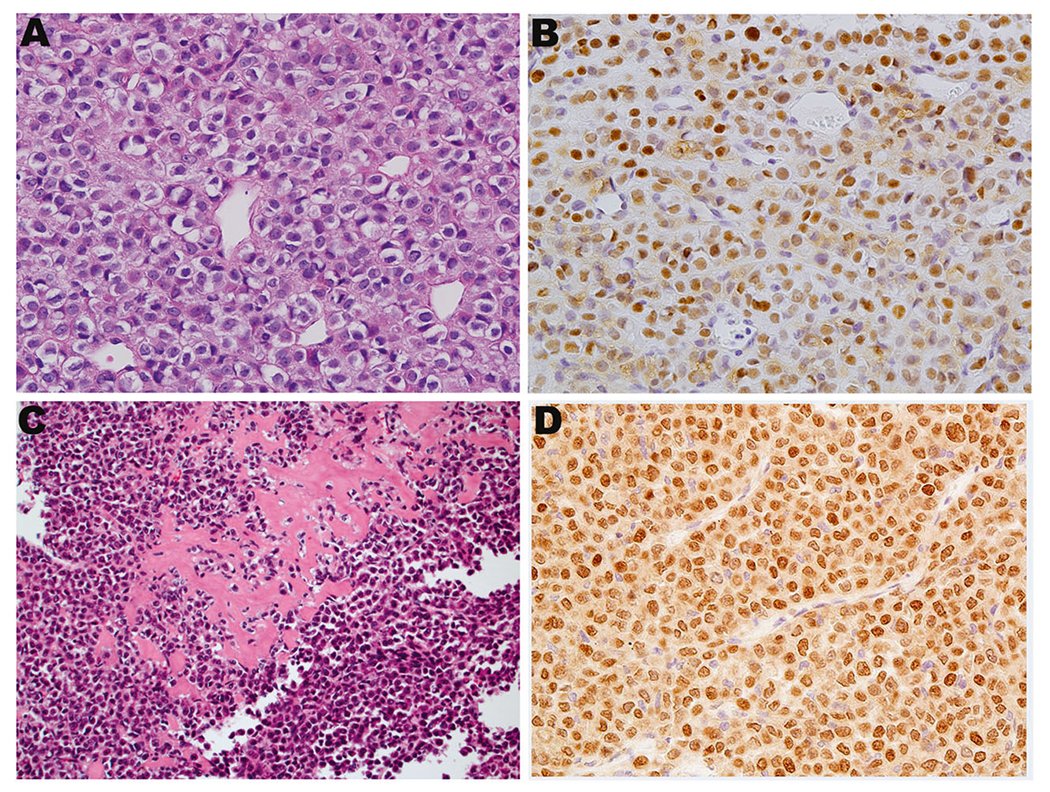
36/ SDH-deficient GISTs almost always occur in the stomach, usually in younger patients. They are usually multinodular and epithelioid on histology. Unlike most other GISTs, this form is in fact willing to metastasize to lymph nodes (pics 2-3).

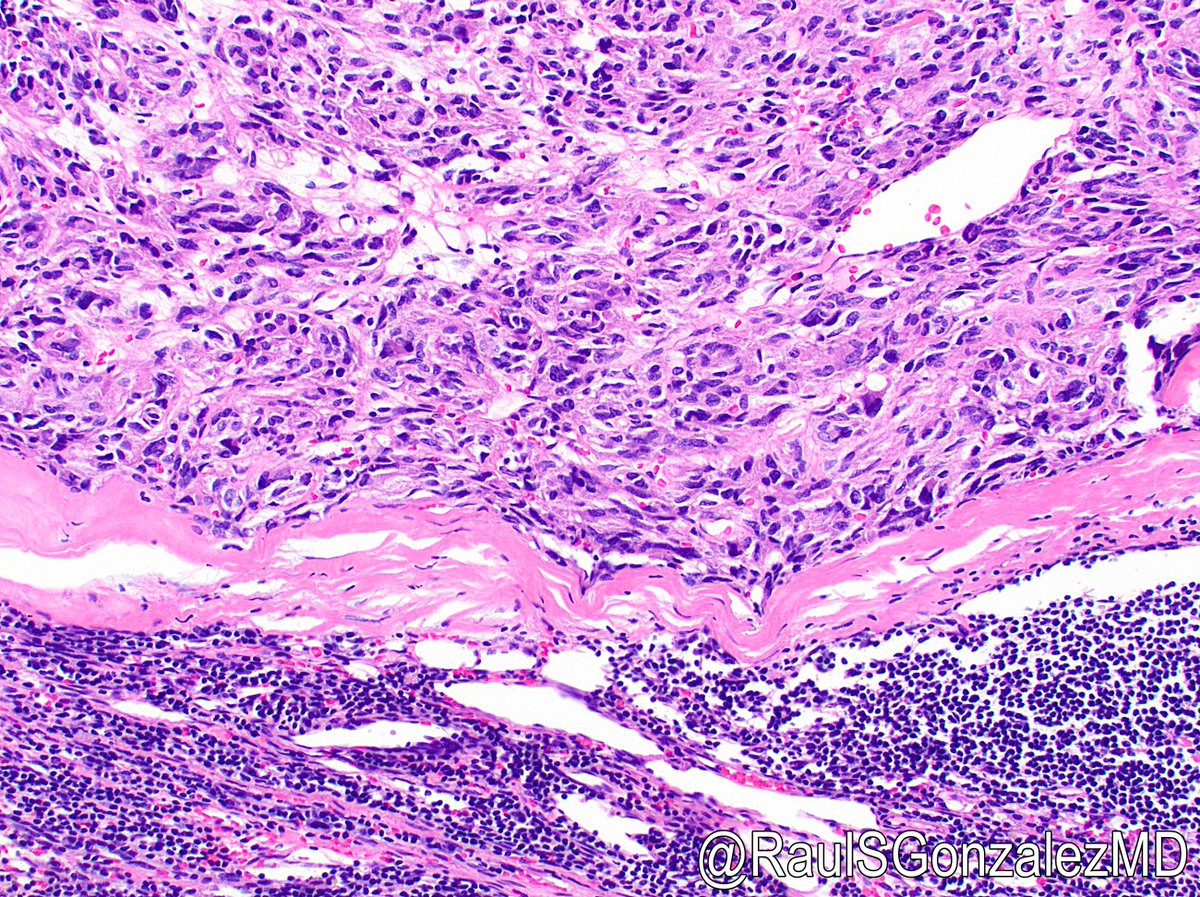
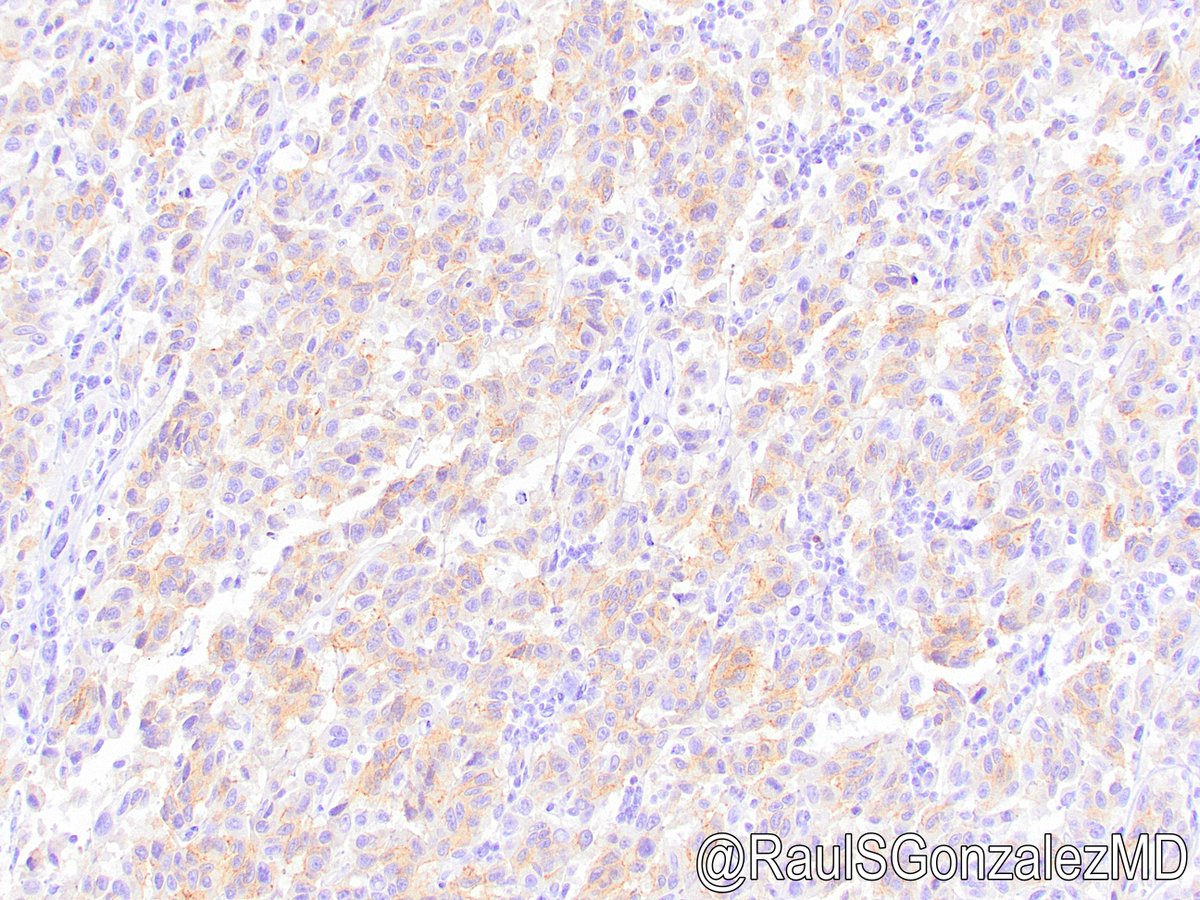
37/ Bad news: SDH-deficient GISTs don’t “follow the textbook” when it comes to risk stratification. Using size and mitotic criteria doesn’t seem to predict how they’ll do. Good news: They almost always do well! They also lose SDHB expression by IHC.


38/ SDH-deficient GISTs often arise in the setting of Carney-Stratakis syndrome (GIST + paraganglioma; autosomal dominant SDH germline mutation) or Carney complex (GIST + paraganglioma + pulmonary chondroma; not familial).
39/ Getting into the rare stuff … patients with neurofibromatosis type 1 can develop GISTs with NF1 mutations. These often affect the small bowel and can be strikingly multifocal (see gross pics). Low risk for progression, fortunately.



40/ A small percentage of GISTs (maybe 2%) can harbor BRAF V600E mutations. This is most notable because it confers imatinib resistance.
41/ Finally, there’s “none of the above.” Quadruple wild-type GISTs lack mutations in KIT, PDGFRA, BRAF/RAS/NF1, and SDH complex genes. It’s looking like some of these show increased FGF4 expression.
42/ That’s the current story for molecular underpinnings. As GISTs progress and act nasty, however, a whole lot of additional genes can develop mutations, including familiar faces such as CDKN2A, TP53, and RB.
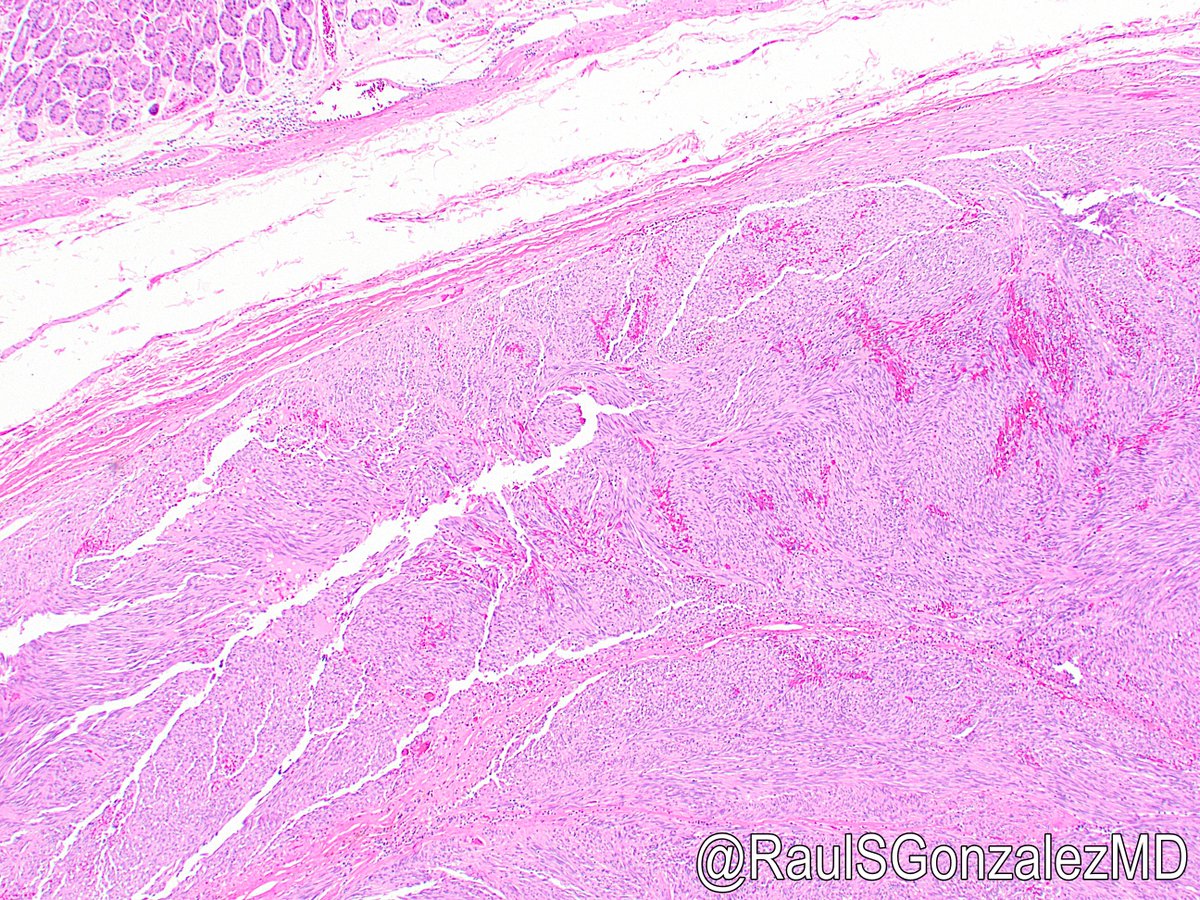
43/ Now let’s talk about tips, tricks, and pitfalls when reviewing GISTs for signout. Sometimes, you’ll get cases following neoadjuvant therapy. This can cause a lot of changes, including myxoid change, necrosis, and paucicellular regions.



44/ Other times, therapy makes GIST strikingly pleomorphic and/or abruptly dedifferentiated (pics 1-2, ref: bit.ly/3cuEouu). To be fair, pleomorphism can also occur in non-treated GISTs, usually epithelioid ones that have progressed (pic 3, ref: bit.ly/3PyFioz).



45/ In contrast, some GISTs are so small and bland that they are discovered incidentally in resection specimens. These “seedling GISTs” (or “baby GISTs”) are usually in the upper GI tract and are basically always benign. bit.ly/3zxr2qx


46/ Another fun little finding seen in the occasional GIST is ossification. It’s probably worth assuming such GISTs have been there a long time and are unlikely to cause further trouble to the patient.

47/ I mentioned earlier that GISTs can show atypia and also vacuolization. In extreme examples, this can mimic signet ring change.

48/ Another interesting but rarely encountered finding in GISTs is entrapment of the overlying mucosa. Don’t mistake it for an invasive adenocarcinoma!
49/ Of course, on rare occasions, you can in fact have an adenocarcinoma or another tumor within a GIST. These amazing pics show an appendiceal goblet cell adenocarcinoma metastasizing to a GIST (thank you to Dr. Altaf Taher for this case!).

50/ Final tip. Is it worth trying to risk-stratify GIST on small biopsy samples, when true mitotic rate is unclear and size info comes from imaging? Seems it’s often accurate, though of course not always, and may not impact management: bit.ly/3zxsLMw

51/ Let’s end this Tweetorial with a discussion of differential diagnoses. GISTs are among the most common mesenchymal neoplasms of the digestive tract, so you should always consider them, but several things can mimic GIST to varying degrees.
52/ First, smooth muscle tumors. Leiomyoma is common and can form small polyps or large mural masses (pic 1). They are usually very pink and bland histologically (except the rare symplastic variant, see pic 2). SMA and desmin are positive.


53/ GI tract leiomyosarcoma is rare and aggressive. Atypia and mitoses are common. Smooth muscle differentiation may be less obvious on H&E, but SMA and desmin are positive. There is a recent paper on malignancy criteria: bit.ly/3d0RIHw


54/ Schwannoma is another important differential for mural mesenchymal masses. Keep in mind that GI tract schwannomas are less likely than their soft tissue counterparts to have prominent palisading and thick-walled blood vessels.

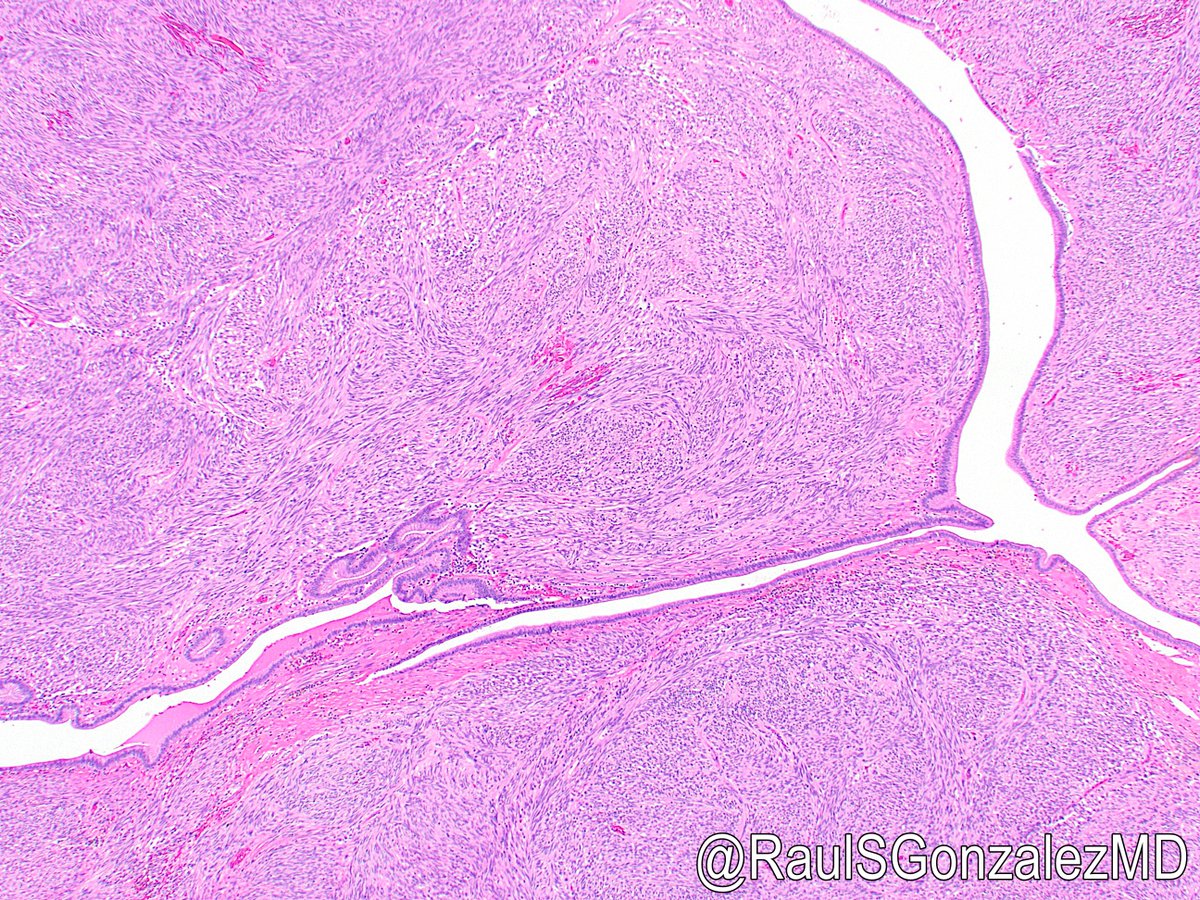
55/ GI tract schwannomas often have a prominent lymphoid cuff, which is helpful but not specific. Compare pic 1 (schwannoma) and pic 2 (GIST)! S100 IHC will confirm the diagnosis of schwannoma for you.


56/ Inflammatory fibroid polyp arises in the submucosa rather than the muscularis propria. It can often be diagnosed on H&E, given the prominent eosinophils and the characteristic onion-skinning of lesional cells around blood vessels.

57/ Don’t be fooled – IFP has some overlap with GIST, including spindled cells, CD34 positivity (pic), and PDGFRA mutations. They are fortunately negative for KIT and DOG1 by immunohistochemistry. These do not metastasize.

58/ Calcifying fibrous pseudotumor can create a bland, paucicellular mass in the wall of the GI tract with associated inflammation. IHC is nonspecific. Calcification is a nice clue but not always present. Ref: bit.ly/3pBBgR0


59/ More interesting is gangliocytic paraganglioma (or “composite gangliocytoma/neuroma and neuroendocrine tumor” per the new endocrine WHO blue book). This weird triphasic lesion almost always occurs in the ampulla and rarely metastasizes.
60/ This entity is usually suspected on H&E and shows spindled Schwannian cells, epithelioid endocrine cells, and scattered ganglion cells. If spindle cells predominate, it could mimic GIST, but IHC for neuroendocrine markers and S100 help confirm the diagnosis.



61/ There are other bland mesenchymal stromal polyps in the GI tract, such as perineurioma (pic 1, GLUT1 positive) and Schwann cell hamartoma (pic 2, S100 positive). These are very unlikely to be mistaken for GIST, but you never know.


62/ One exception is Kaposi sarcoma, which pops up now and then in the GI tract. Several histologic patterns have been reported, including an uncommon GIST-like form (recent ref: bit.ly/3w744V9). HHV8 of course confirms the diagnosis.


63/ Solitary fibrous tumor is rare in the GI tract but can certainly occur. They also form mural masses. They demonstrate the characteristic “patternless pattern” of lesional cells, along with classic branching staghorn blood vessels.


64/ SFT is also CD34-positive – so don’t rely on that stain in isolation! They are positive for STAT6 (pic) and negative for KIT and DOG1. (I once had a GI tract SFT with nuclear-only DOG1 positivity, which I assume was a weird artifact.)

65/ Another spindle cell neoplasm that can rarely arise in the GI tract and maybe mimic GIST is follicular dendritic cell sarcoma. These show prominent nucleoli, moderate N:C ratio, and a brisk lymphocytic infiltrate. They’re positive for CD21, CD25, CD35, and sometimes EBV.

66/ We all know granular cell tumor can arise in the esophagus, but don’t overlook it elsewhere in the GI tract. The pictures show a case from the colon. IHC for S100 and CD68 still confirm the diagnosis. Unlikely to be mistaken for GIST, but not impossible.


67/ If you see a bland spindled proliferation near the GI tract but originating outside it, think of desmoid fibromatosis. It’s composed of long fascicles with “school of fish” nuclei (all going in the same direction). Nuclear beta-catenin IHC is often positive but may be focal.


68/ Melanoma is very rare as a primary GI tract lesion but can certainly metastasize there. They are often quite ugly and can mimic a high-grade epithelioid GIST. If you’re lucky, you will see intralesional pigment.

69/ Once again, perform IHC stains to confirm the diagnosis. Melanoma should be positive for at least one melanoma marker (S100, SOX10, HMB45, Melan-A, etc.). Beware -- mucosal melanomas are DOG1-negative but can be KIT-positive (pic)!
70/ Speaking of S100-positive lesions, don’t forget about gastrointestinal neuroectodermal tumor (formerly “clear cell sarcoma-like tumor of the gastrointestinal tract”). It expresses neuroendocrine markers, S100, and SOX10 -- tricky!
71/ This rare, aggressive lesion forms sheets and nodules of epithelioid cells in the wall of the GI tract, with necrosis and occasional giant cells. EWSR1 fusions are characteristic (often with ATF1 or CREB1). It has a poor prognosis. Thanks to Dr. Sabrina Sopha for this case.


72/ Other ugly malignancies may arise in or around the gastrointestinal tract and secondarily involve it, mimicking a high-grade GIST. Examples include undifferentiated pleomorphic sarcoma (pics 1-2) and dedifferentiated liposarcoma (pics 3-4).



73/ Getting into some weird stuff at the end. Cajal cell hyperplasia can sometimes form a vague, angulated lesion that is not quite a GIST. KIT and DOG1 positive. I’m not aware of this rare process ever metastasizing.

74/ Plexiform fibromyxoma (née plexiform angiomyxoid myofibroblastic tumor) is a rare benign gastric neoplasm with distinctive architecture and low-grade morphology. IHC is nonspecific, though some cases harbor a MALAT1-GLI1 fusion. Remember GLI1; I’ll mention it again in a bit.


75/ Finally, let’s discuss three relatively new molecularly defined mesenchymal lesions that can arise in the GI tract. First, NTRK-rearranged mesenchymal neoplasms of the GI tract. These vary in terms of site, patient age (often young), and clinical outcome.
76/ They show NTRK gene fusions and are positive for pan-TRK IHC. Histologic patterns include infantile fibrosarcoma-like, low-grade CD34- and S100-positive (pics, courtesy of Dr. Lindsay Alpert), and high-grade. Ref: bit.ly/3vvNDBt


77/ Next, NUTM1-rearranged colorectal sarcoma. They arise in submucosa and often metastasize. Histology: bland spindled or epithelioid cells, sometimes rhabdoid fx and necrosis. IHC positive for keratins and NUT. Ref: bit.ly/3SorIWs
78/ I’ve never (knowingly) seen a case. One published series of NUTM1-rearranged neoplasms included one colon case; it’s freely available in PMC, so pictures of a non-colon case from that paper are shown here. Ref: bit.ly/3dahV6c

79/ Last and least (since they’re ridiculously rare) is GLI1-rearranged enteric tumor. They variably show areas of oval/spindled cells and/or keratin-positive epithelioid cells. “Gastroblastoma” arguably fits under this heading. Recent ref of 3 cases: bit.ly/3JZy4Id


80/ That’s it for this whirlwind tour and my longest Tweetorial yet! I hope people found this helpful. Any questions or comments, feel free to reply to this thread. Also, please mash that subscribe button! (Oh, wait, wrong platform.)
• • •
Missing some Tweet in this thread? You can try to
force a refresh