@rex_steffen speaks on cardiac disease in #OBAnes at #OAA3dc2022, setting the expectations immediately (we haven’t got all week) - for a complete list, read escardio.org/Guidelines/Cli…. 



@rex_steffen starts with a case study… I think the pause was echoed by ALL the #OBAnes in the room at #OAA3dc2022

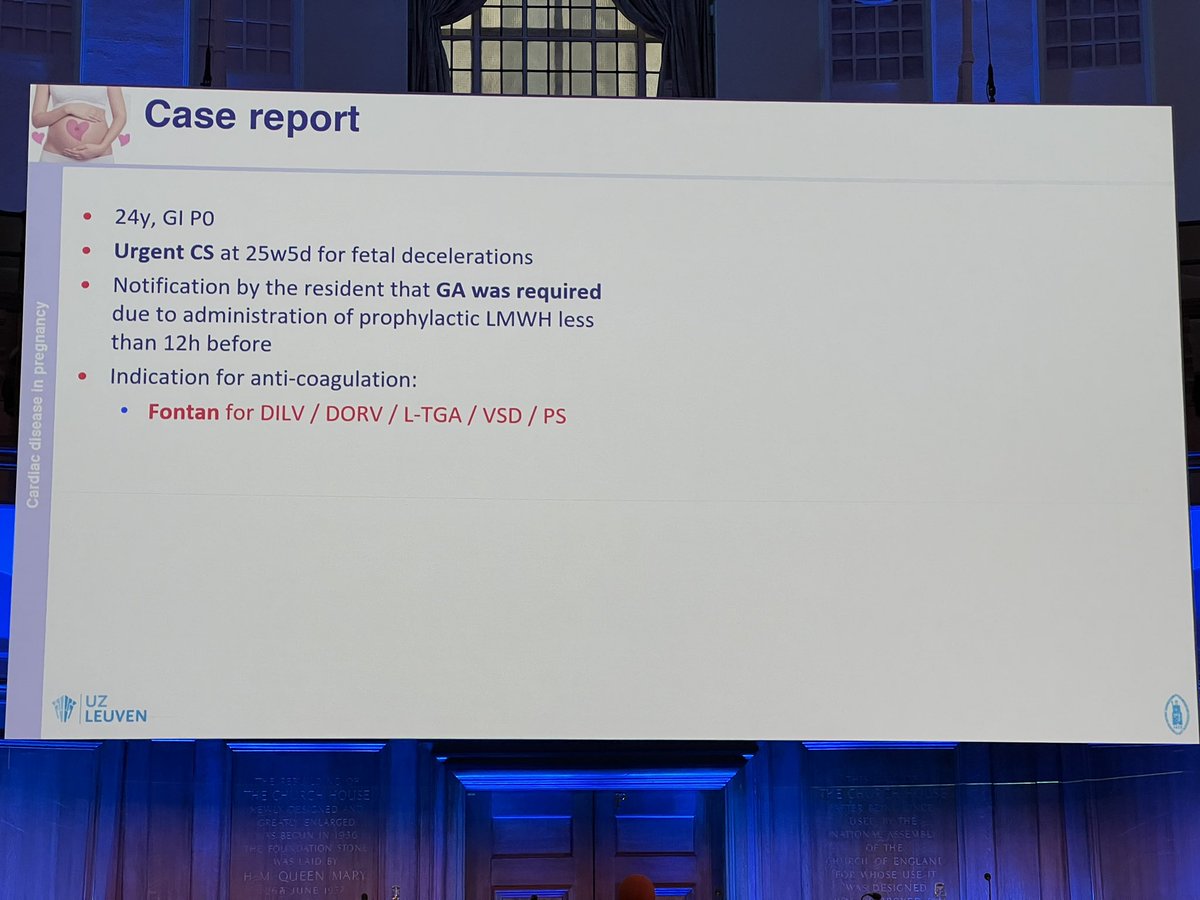

Great Fontan video… cesarean uneventful, patient required reintubation for second GA because of her heart - doing the potentially difficult airway twice? No thanks! #OAA3dc2022 twitter.com/i/web/status/1…
@rex_steffen continues with epidemiology. Cardiac disease 0.2-4% pregnancies & increasing. Acquired/ modifiable factors exist. Adult congenital heart disease = most common heart disease in pregnancy.
#OAA3dc2022
#OAA3dc2022



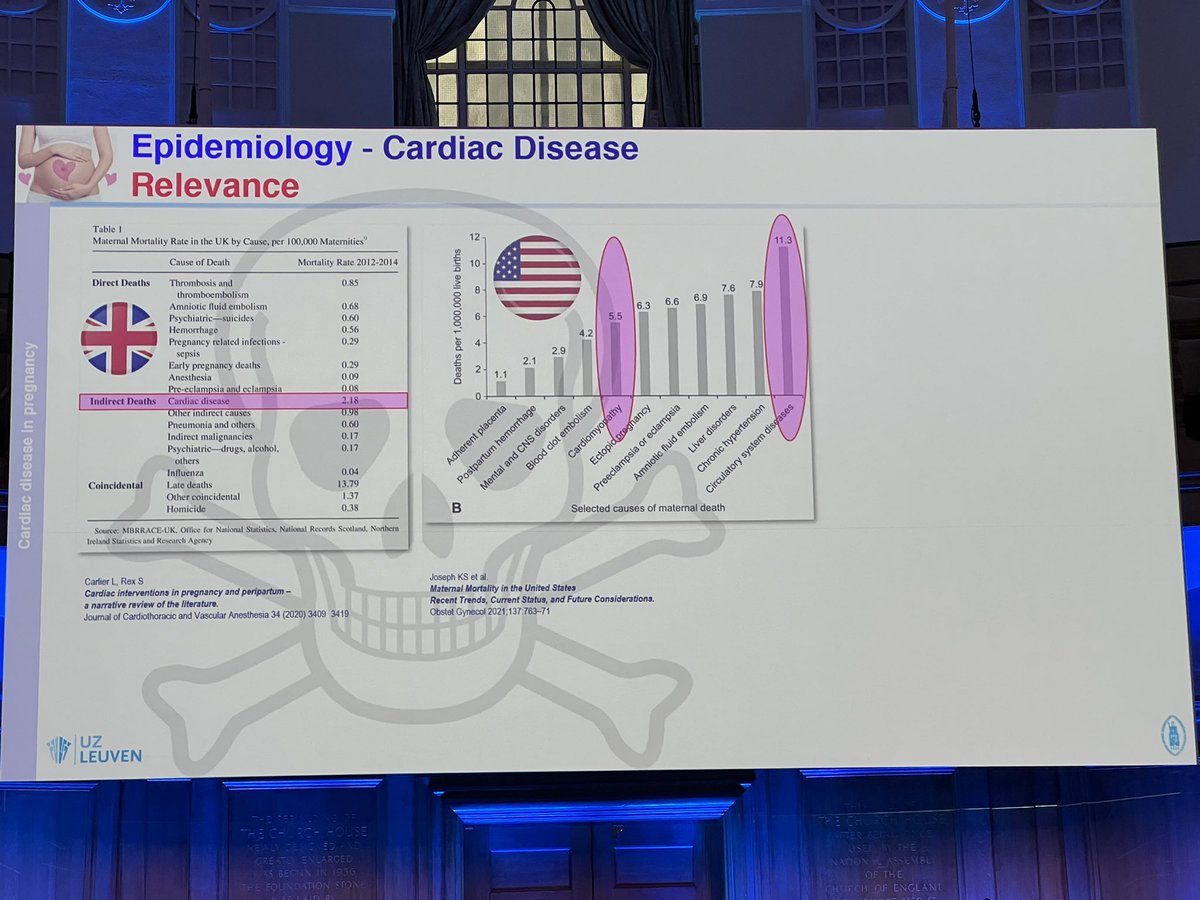
Relevance of cardiac disease = leading cause of death.
MOST importantly, while everything else seems to be improving (downward trend), cardiac deaths are INCREASING.
Only 17% women have pre-existing diagnosis - highly level of suspicion required
#OAA3dc2022
MOST importantly, while everything else seems to be improving (downward trend), cardiac deaths are INCREASING.
Only 17% women have pre-existing diagnosis - highly level of suspicion required
#OAA3dc2022



Why is cardiac disease so dangerous in pregnancy? The second heart beat, may topple the first. Pregnancy and labour stress CVS. When do they die? 23-34 weeks and postpartum weeks 1-4. Cardiac disease & standard OB meds are incompatible #OAA3dc2022




Both oxytocin and carbetocin decrease MAP 25%. Phenylephrine decreases cardiac output - is there any to spare? How dangerous is cardiac disease - lowest risk adverse event = 2.5-5%. Fine tuning risk prediction: CARPREG, ZAHARA, ROPAC - structural & functional issues
#OAA3dc2022
#OAA3dc2022




Who should be in charge of management? Longitudinal multidisciplinary multidimensional team = best. Timing & delivery - most vaginal. Cesarean still OB domain.
The @Eltonchris list - No wrong anesthetic, but many ways to give a bad anesthetic.
How blood flows = NB
#OAA3dc2022
The @Eltonchris list - No wrong anesthetic, but many ways to give a bad anesthetic.
How blood flows = NB
#OAA3dc2022




Key hemodynamic issues - the basics are still the basics.
RA has been used for all cardiovascular disease - low dose, titratable RA preferred. GA patients generally sicker, poorer fetal outcomes. 4 pillars of heart failure Mx contraindicated in pregnancy
#OAA3dc2022
RA has been used for all cardiovascular disease - low dose, titratable RA preferred. GA patients generally sicker, poorer fetal outcomes. 4 pillars of heart failure Mx contraindicated in pregnancy
#OAA3dc2022




Therapeutic options when medical management fails - @rex_steffen algorithm. ECMO is much better than its reputation.
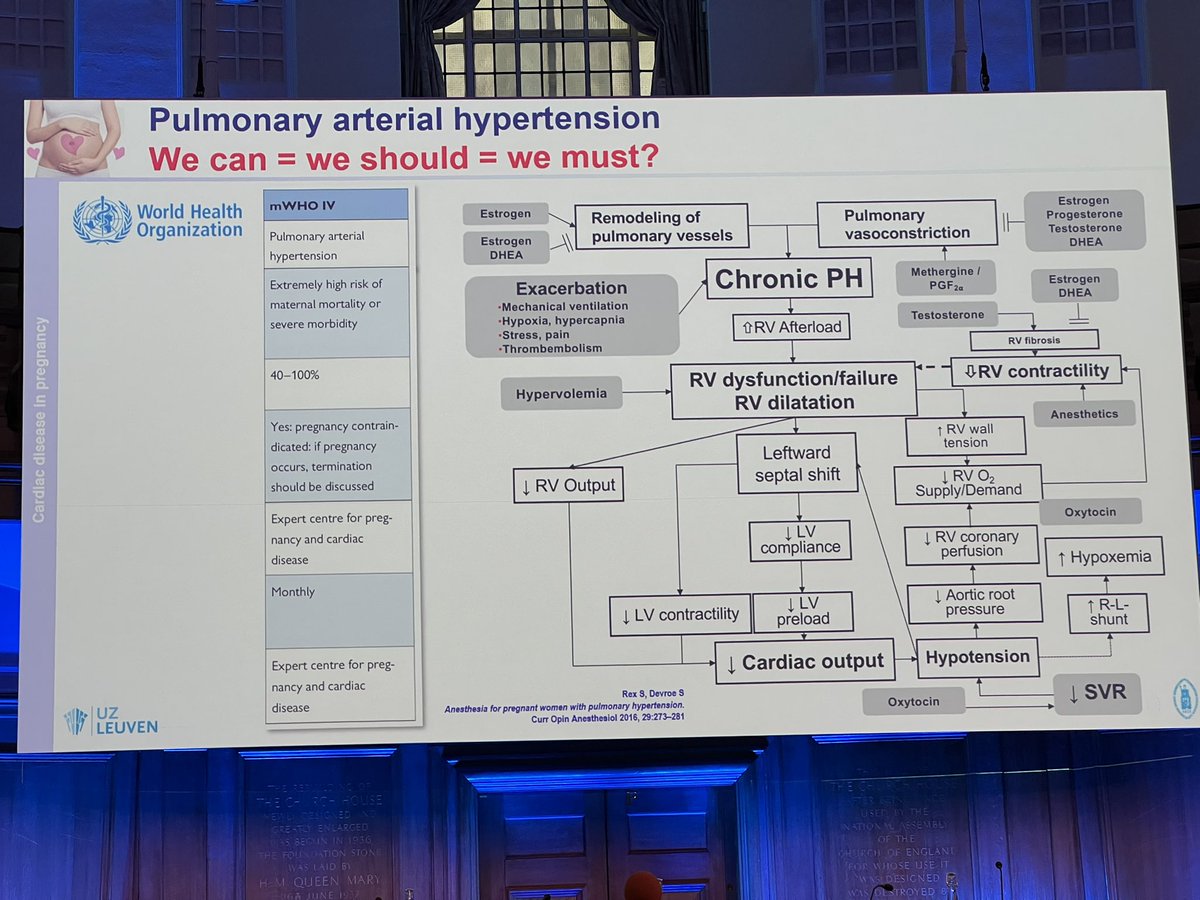
We can = we should = we must? It’s complicated, almost invariably bad. Emotions vs reality. Mom > fetus - treat mom first.
#OAA3dc2022
We can = we should = we must? It’s complicated, almost invariably bad. Emotions vs reality. Mom > fetus - treat mom first.
#OAA3dc2022



Excellent conclusion/ summary slide from @rex_steffen on cardiac disease in pregnancy at #OAA3dc2022


@threadreaderapp unroll please
• • •
Missing some Tweet in this thread? You can try to
force a refresh