
Thousands have made the jump from #MedTwitter to #MedMastodon!
One issue I’ve heard is “I can’t get the app to work” or “I can’t find the server”
Good news: there are many mobile apps to choose from. Personally I think Meta-text & Tooot are easier to setup.
Here’s how.🧵
1/
One issue I’ve heard is “I can’t get the app to work” or “I can’t find the server”
Good news: there are many mobile apps to choose from. Personally I think Meta-text & Tooot are easier to setup.
Here’s how.🧵
1/
1️⃣ Setup a #MedMastodon account:
The easiest way is just follow this invite
med-mastodon.com/invite/JLmsx3H6
You should see something like this.👇
Choose a name (or “handle”), enter your email address, & makeup a (secure) password.
That’s it!
2/
The easiest way is just follow this invite
med-mastodon.com/invite/JLmsx3H6
You should see something like this.👇
Choose a name (or “handle”), enter your email address, & makeup a (secure) password.
That’s it!
2/

Once you confirm your email you should be able to login through the browser. Done
2️⃣If you prefer an app, you can choose from many options in the App Store.
Personally, I like Metatext; it’s open source, free, no ads, & doesn’t collect any user data!
apps.apple.com/us/app/metatex…
3/
2️⃣If you prefer an app, you can choose from many options in the App Store.
Personally, I like Metatext; it’s open source, free, no ads, & doesn’t collect any user data!
apps.apple.com/us/app/metatex…
3/
3️⃣ Download the app from the App Store.
4/
4/

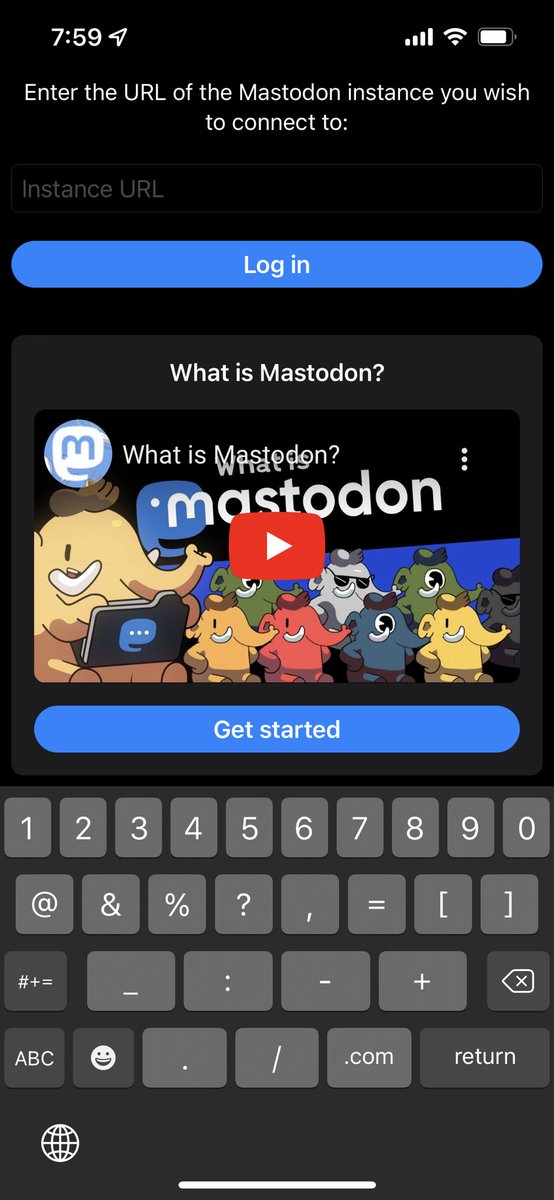
4️⃣ Open the app and enter the name of your server where it says “instance URL”
If you created an account at #MedMastodon (step 1️⃣ in this tweetorial) you should fill in “med-mastodon.com”
⚠️ be careful to include the dash
Click login
If you created an account at #MedMastodon (step 1️⃣ in this tweetorial) you should fill in “med-mastodon.com”
⚠️ be careful to include the dash
Click login

5️⃣ Enter the handle & password you chose in step 1️⃣
(if you are already logged in through the browser on your phone it may skip this step 😁)
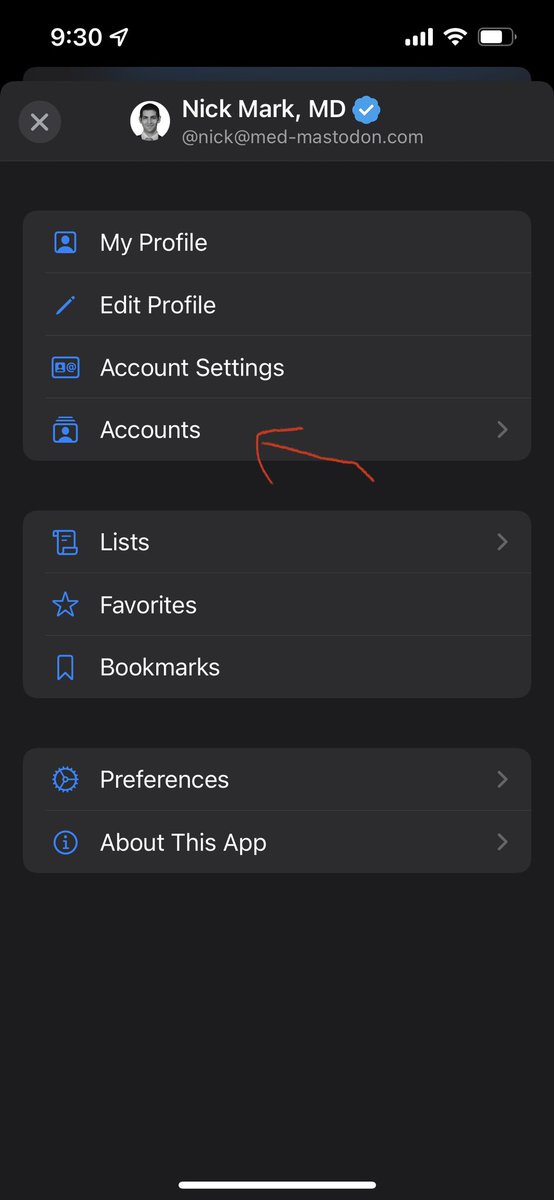
🆒 Bonus: you can connect to multiple Mastodon accounts via Metatext. If you have another account that you want to keep, just add it
6/
(if you are already logged in through the browser on your phone it may skip this step 😁)
🆒 Bonus: you can connect to multiple Mastodon accounts via Metatext. If you have another account that you want to keep, just add it
6/

That’s it! Take a look 👀
The Mastodon experience is a lot like Twitter… with a few things that make it better IMO: Small self moderated, no hate speech/misinformation, no algorithm, just a feed
(If there’s interest I’ll do an explainer about some of the differences.)
7/7
The Mastodon experience is a lot like Twitter… with a few things that make it better IMO: Small self moderated, no hate speech/misinformation, no algorithm, just a feed
(If there’s interest I’ll do an explainer about some of the differences.)
7/7
• • •
Missing some Tweet in this thread? You can try to
force a refresh































