1/ We want to improve haemodynamic management and fluid stewardship at my place (Honvédkórház ICU, Budapest, Hungary).
See examples of study metrials below and please tear them apart as we want to improve them further.
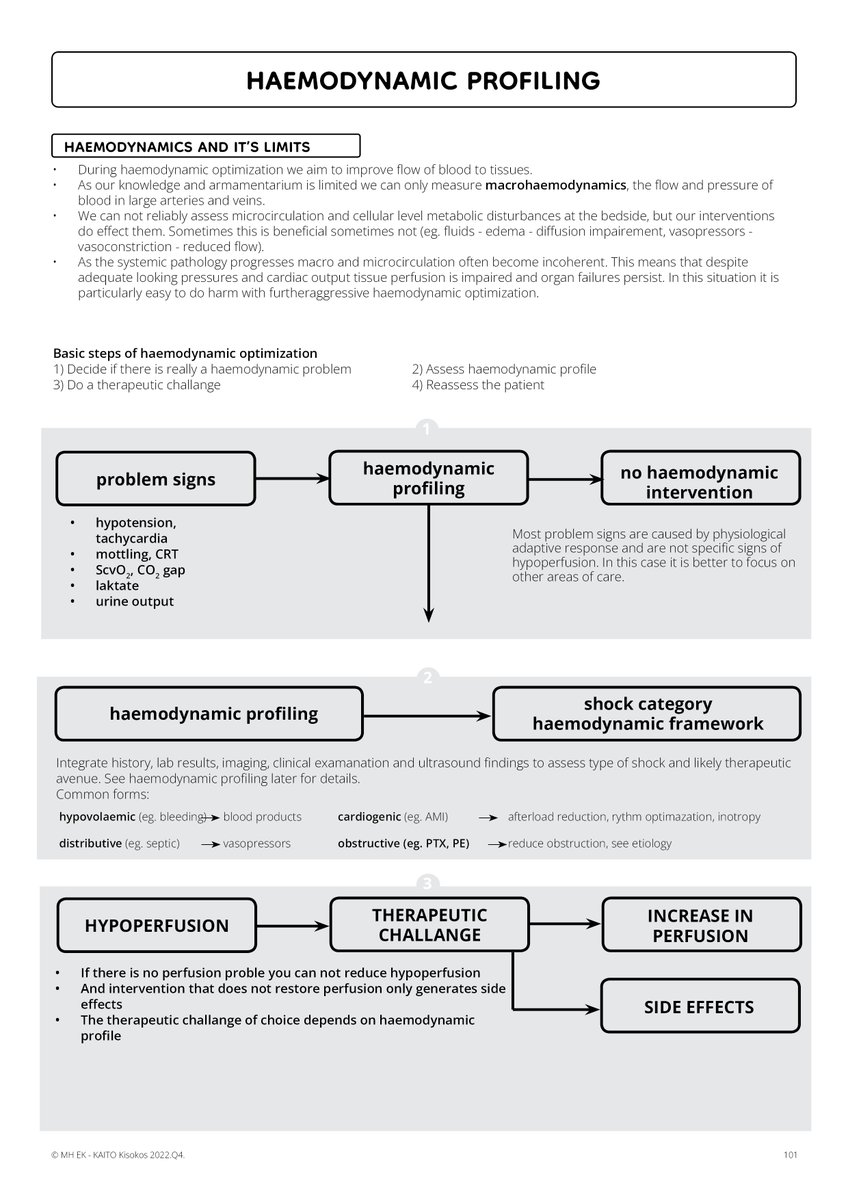
The first one was made to avoid reflex fluids in oliguria.
See examples of study metrials below and please tear them apart as we want to improve them further.
The first one was made to avoid reflex fluids in oliguria.

2/ Inspired by #HR2022 @AndromedaShock @khaycock2 @ThinkingCC @msiuba
@PulmCrit @iceman_ex @icmteaching and many more. Thank you all!
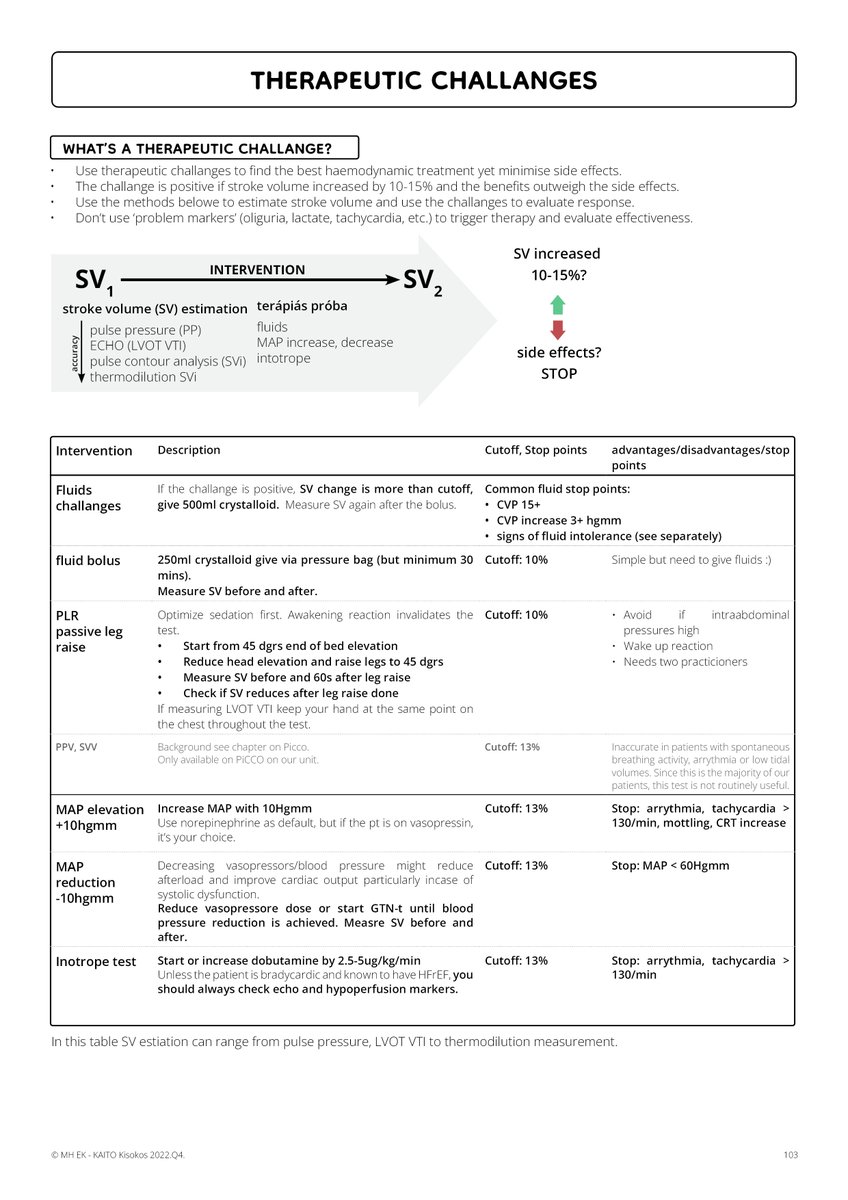
The rest of the pages are about haemodynamic profiling.
@PulmCrit @iceman_ex @icmteaching and many more. Thank you all!
The rest of the pages are about haemodynamic profiling.
3/ Notes
- The target population is an ICU doc with a few years of experience with variable US skills.
- implementation will be with hands-on training
- This is an excerpt from a 12-page long document but did not have the time to translate all
- The target population is an ICU doc with a few years of experience with variable US skills.
- implementation will be with hands-on training
- This is an excerpt from a 12-page long document but did not have the time to translate all

4/
- excuse my translation and spelling please
- many things are very much local, e.g. we use lots of PiCCO but no Swans, most of our patients are trauma/burns/postsurgical with some medical
- NA stands for norepinephrine in ug/kg/min
- excuse my translation and spelling please
- many things are very much local, e.g. we use lots of PiCCO but no Swans, most of our patients are trauma/burns/postsurgical with some medical
- NA stands for norepinephrine in ug/kg/min
• • •
Missing some Tweet in this thread? You can try to
force a refresh