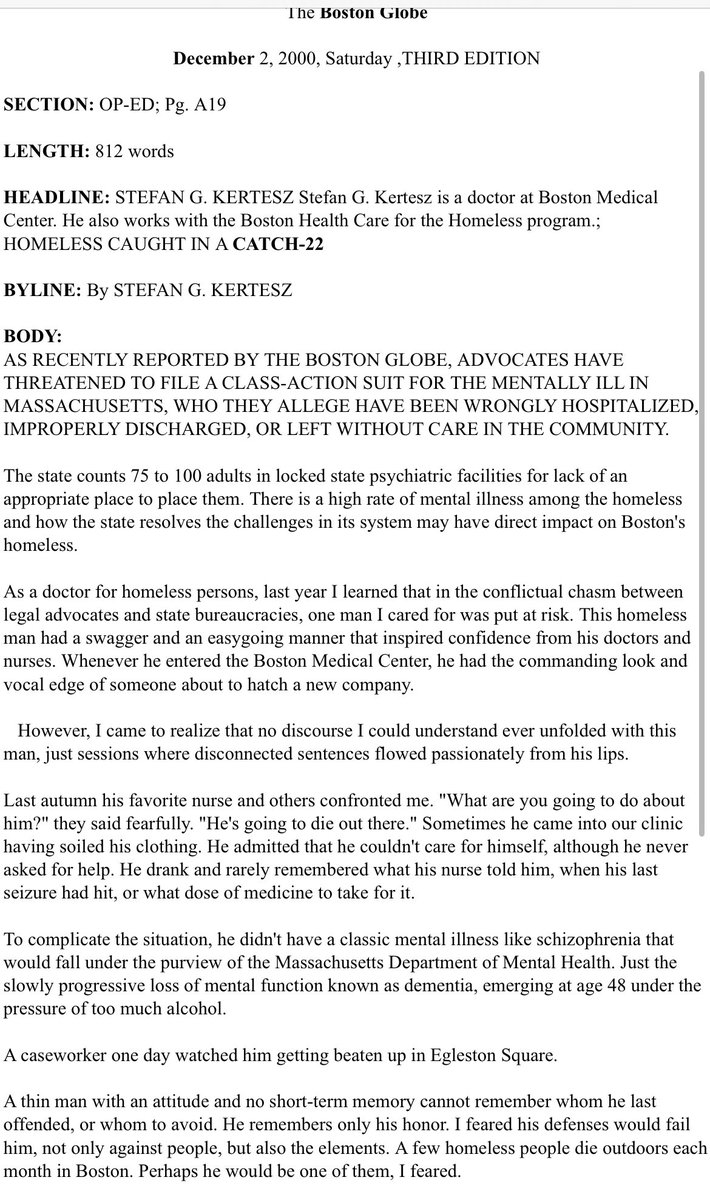
1/22 years ago I wrote in the Boston Globe about my fear for the survival of my #homeless patient who was mostly demented, alcoholic, and often beaten up on the streets.
I have that in mind as we see reactions to New York’s plans to deploy an involuntary confinement response
I have that in mind as we see reactions to New York’s plans to deploy an involuntary confinement response

2/That my patient would die was the concern brought to me by nurses who had heard from case workers who had seen him preyed upon.
What I discovered was that there was no path to protect him
What I discovered was that there was no path to protect him
3/Mental health professionals, including a neuropsychologist, agreed that despite some common sense, my patient was completely unsafe
However - in Boston- there was no place empowered legally to hold him. Indeed civil rights advocates were litigating to make sure we never could
However - in Boston- there was no place empowered legally to hold him. Indeed civil rights advocates were litigating to make sure we never could
4/With that in mind, I would caution that when we consider the current New York plan from its Mayor, which seems to involve police & caseworkers, we ask what is valid in that plan and what could wind up being quite bad
5/With 22 years of homeless scholarship and clinical work, it still seems wrong to me that when there is uniform agreement that a homeless patient lacks mental capacity to survive against elements & assault, we do not protect that life.
But that is not quite the end of this
But that is not quite the end of this
6/I do not believe that the political momentum on this matter reflects a sudden discovery of the value of protecting life.
In most cities there is an implied political promise: that the new police powers will solve homelessness or make frustrated homeowners’ lives easier.
In most cities there is an implied political promise: that the new police powers will solve homelessness or make frustrated homeowners’ lives easier.
7/In cities with high levels of street homelessness, the percentage who will fit the profile of my demented patient of 2000 is low. The number of persons homeless in any community is driven primarily by community rents. Hospital beds (even 50 of them) will not change that
8/So, where the political justification is to make the streets look nice, there are two obvious problems: the forced hospital policy will not achieve that,
and it is a diversion from addressing the problem of people who are poor or needy having no long term rentable option
and it is a diversion from addressing the problem of people who are poor or needy having no long term rentable option
9/For most people with a serious mental illness who lack income, they actually are likely to get a housed outcome if a Housing First approach - combining an actual permanent unit + active clinical support - is offered. The biggest barriers are 2-fold
10/1st, Many cities/counties see no way to overcome the lack of affordable rentable units, which result from (a) zoning limitations chosen by their own citizens
(b) US tax policies that prioritize housing subsidies for mortgages far above affordable housing for the poor
(b) US tax policies that prioritize housing subsidies for mortgages far above affordable housing for the poor
11/efforts to present Housing First favorably, from some advocates, tend to underplay the need for robust, well-funded clinical support that requires very active engagement. This creates a situation of dashed expectations, which I have described
12/For a small group, I support a city-level response that assures direct intervention -which may not be consensual- for a person who is at very risk of dying because of hallucinations or dementia.
But no data suggest the police can deliver this safely
But no data suggest the police can deliver this safely
13/If the average citizen is just saying “there are too many homeless people”, please realize that the core problem is some combination of your housing & rental market, your zoning choices, your geography & the differential allocation of support for homeowners with mortgages
14/For people who wish to see the full column I wrote for the Boston Globe roughly 22 years ago, I am only sharing a part publicly as it seems to be copyright protected. I can share privately on request
• • •
Missing some Tweet in this thread? You can try to
force a refresh