Reason # 67543 why #pocus is important: sometimes mild symptoms are a sign of impending disaster.
41 year old thin athletic male presented to the hospital with a few weeks of mild shortness of breath with exertion.
BP 170/70, HR 100. CXR with cardiomegaly, tortuous aorta.
41 year old thin athletic male presented to the hospital with a few weeks of mild shortness of breath with exertion.
BP 170/70, HR 100. CXR with cardiomegaly, tortuous aorta.
Bedside #pocus exam shown below:
Most glaring is the size of the aorta. It is clearly larger than the left atrium. Also notable is the anterior leaflet of the mitral valve isn’t opening much.
This is either due to mitral stenosis, systolic heart failure or aortic regurgitation. Placing color Doppler on the valve gives you the answer.
So in about 1-2 minutes we have a good idea what’s going on here: thoracic aortic aneurysm with severe aortic regurgitation. Measuring the aortic root and thoracic aorta confirms the diagnosis. 

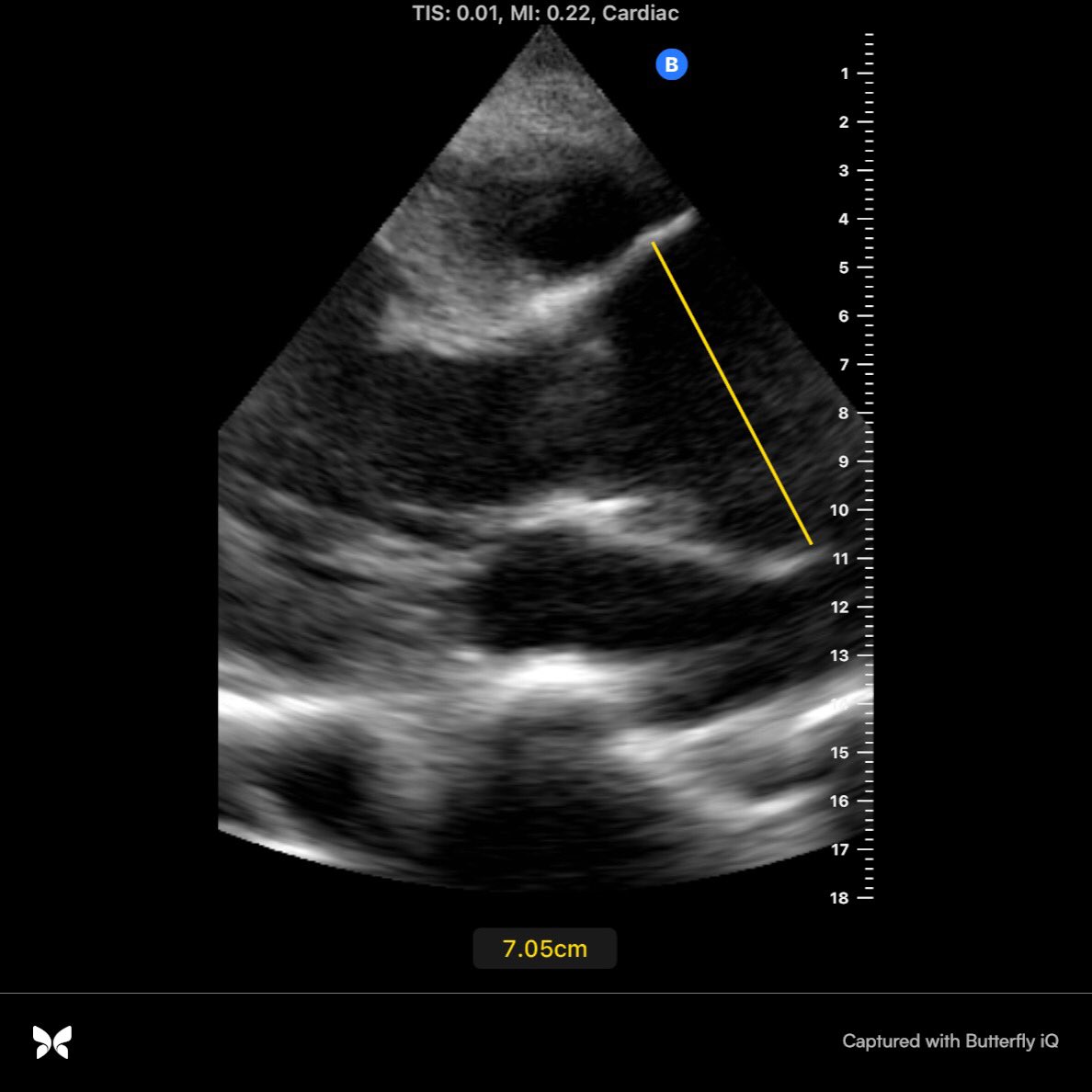
This is a pending surgical emergency waiting to happen. Even with auscultation and detecting a diastolic murmur it isn’t until such images are obtained that the surgeons will come running.
We are saddened by the passing of the sports journalist Grant Wahl. When we heard it was due to a ruptured ascending aortic aneurysm we couldn’t help but wonder if it could have been detected with #pocus. He reportedly sought medical attention twice that week.
We will never know but certainly #pocus could have, or detected a pericardial effusion, enlarged aortic root, etc. This is also sadly how actor John Ritter died:
pocusmeded.com/post/could-poc…
pocusmeded.com/post/could-poc…
@NephroP @POCUS_Society @RJonesSonoEM @UAlberta_Sono @IM_POCUS @TaotePOCUS @nilamjsoni #foamed #meded #cardiotwitter @iceman_ex
• • •
Missing some Tweet in this thread? You can try to
force a refresh