Autonomous Sensory Zones
(peripheral nerves)
Median nerve illustration by Guttmann (1939)
#MedTwitter #neurotwitter #EndNeurophobia #tweetorials
1/
(peripheral nerves)
Median nerve illustration by Guttmann (1939)
#MedTwitter #neurotwitter #EndNeurophobia #tweetorials
1/

Definition
“regions where single nerve roots supply distinct and non-overlapping areas of skin”
- small portion of dermatome
- few nerve roots have such autonomous zones
- great variability
2/
“regions where single nerve roots supply distinct and non-overlapping areas of skin”
- small portion of dermatome
- few nerve roots have such autonomous zones
- great variability
2/
Sensory zones
a.maximal zone: maximal area supplied by a peripheral nerve
- maximal=intermediate+autonomous
b.intermediate zone: area of overlap of the maximal zone of different peripheral nerves
c.autonomous zone: area exclusively supplied by a particular peripheral nerve
3/
a.maximal zone: maximal area supplied by a peripheral nerve
- maximal=intermediate+autonomous
b.intermediate zone: area of overlap of the maximal zone of different peripheral nerves
c.autonomous zone: area exclusively supplied by a particular peripheral nerve
3/

Autonomous zones of various nerves:
A. Radial nerve
B. Median nerve
C. Ulnar nerve
D. Common peroneal nerve
E. Sciatic nerve
4/
A. Radial nerve
B. Median nerve
C. Ulnar nerve
D. Common peroneal nerve
E. Sciatic nerve
4/

Radial nerve
area: 1st dorsal web space of hand (Anatomical snuff box)
“according to some authors, radial nerve and common peroneal do not have autonomous zones although complete transection of the nerve results in sensory loss over the mentioned regions”
5/
area: 1st dorsal web space of hand (Anatomical snuff box)
“according to some authors, radial nerve and common peroneal do not have autonomous zones although complete transection of the nerve results in sensory loss over the mentioned regions”
5/

Median nerve
area: distal phalanx (tip) of index finger (2nd finger)
- tip of thumb (other possible area)
6/
area: distal phalanx (tip) of index finger (2nd finger)
- tip of thumb (other possible area)
6/

Ulnar nerve
area: distal phalanx (tip) of little finger (5th finger)
7/
area: distal phalanx (tip) of little finger (5th finger)
7/

Common peroneal nerve
area: central strip on dorsum of foot
“according to some authors, radial nerve & common peroneal do not have autonomous zones although complete transection of the nerve results in sensory loss over the mentioned regions”
8/
area: central strip on dorsum of foot
“according to some authors, radial nerve & common peroneal do not have autonomous zones although complete transection of the nerve results in sensory loss over the mentioned regions”
8/

Sciatic nerve
area: mixed pattern of common peroneal nerve and posterior tibial nerve
9/
area: mixed pattern of common peroneal nerve and posterior tibial nerve
9/

Deep peroneal nerve
area: 1st dorsal web space
10/
area: 1st dorsal web space
10/

Posterior tibial nerve
area: sole of foot
11/
area: sole of foot
11/

Why is important to know the autonomous sensory zones?
“anesthesia in an autonomous zone indicates a complete lesion of that particular nerve”
12/
“anesthesia in an autonomous zone indicates a complete lesion of that particular nerve”
12/
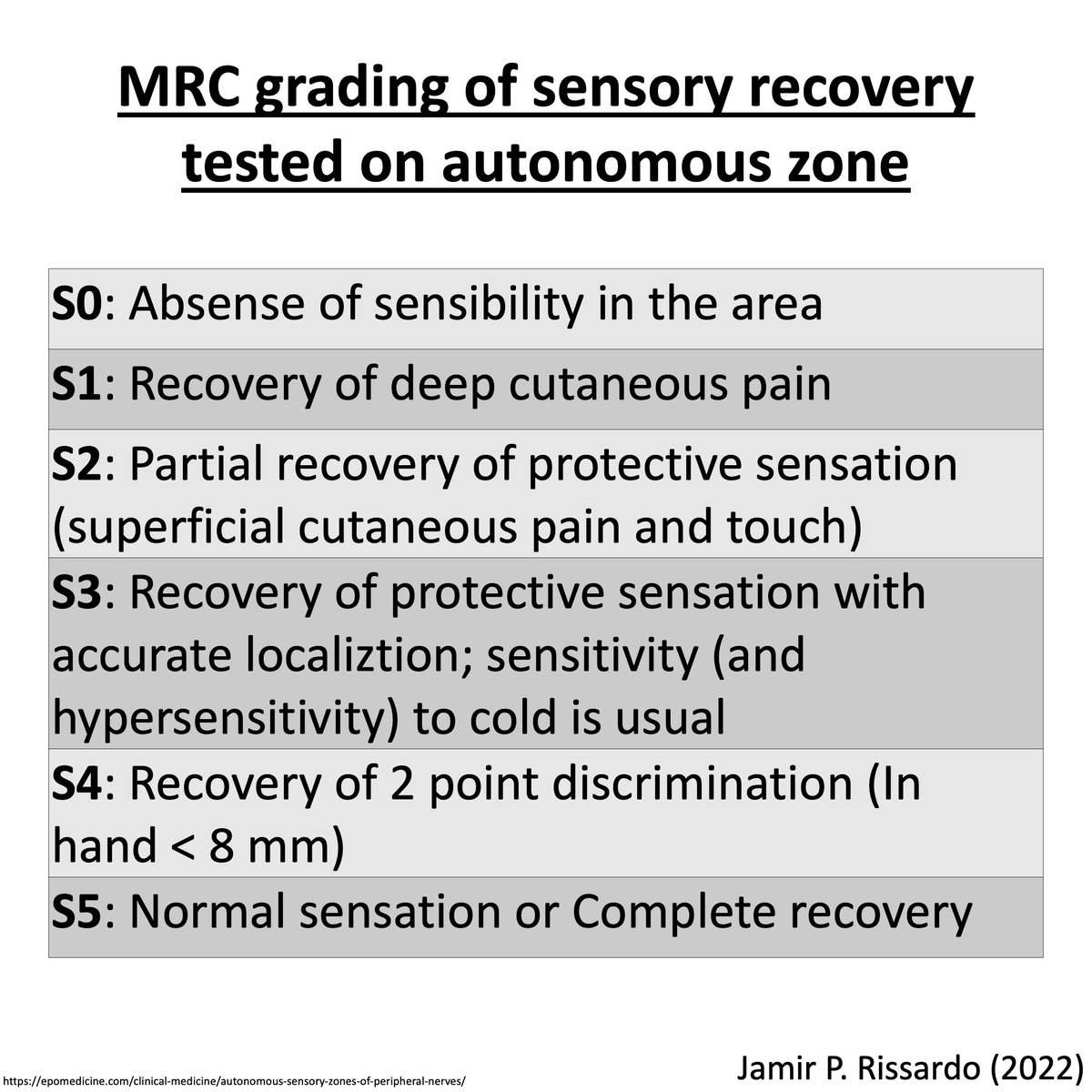
MRC grading of sensory recovery tested on autonomous zone
13/
13/
NeuroTeach - Content
The blog contains all the threads and videos.
neuronland.blogspot.com/2022/11/neurot…
Have a great day!
14/
The blog contains all the threads and videos.
neuronland.blogspot.com/2022/11/neurot…
Have a great day!
14/
• • •
Missing some Tweet in this thread? You can try to
force a refresh