HOLY CHEESE 🧀🧀🧀
I have discovered something that should lead to the immediate investigation of the TGA and every drug regulator
Two FOIs prove that there were batches of #Pfizer vaccine that had killed people and should have failed the batch analysis.
But they kept jabbing.
I have discovered something that should lead to the immediate investigation of the TGA and every drug regulator
Two FOIs prove that there were batches of #Pfizer vaccine that had killed people and should have failed the batch analysis.
But they kept jabbing.
You don't need a science degree or a molecular biology PhD for this. You just need an eye for patterns. Here is FOI 4077 just released.
Each row is a person who died. They died because they believed the TGA ATAGI MHRA JCVI FDA mantra of "safe and effective", which was not true
Each row is a person who died. They died because they believed the TGA ATAGI MHRA JCVI FDA mantra of "safe and effective", which was not true
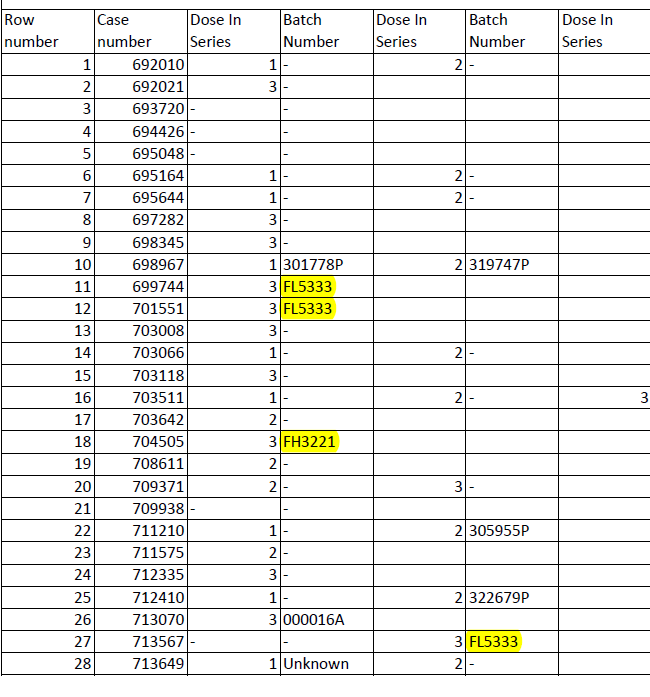
In the report, which is only a fraction of the 900+ deaths reported to the TGA, only a few batch numbers are documented.
Here is the document (it's been archived)
tga.gov.au/sites/default/…
Here is the document (it's been archived)
tga.gov.au/sites/default/…
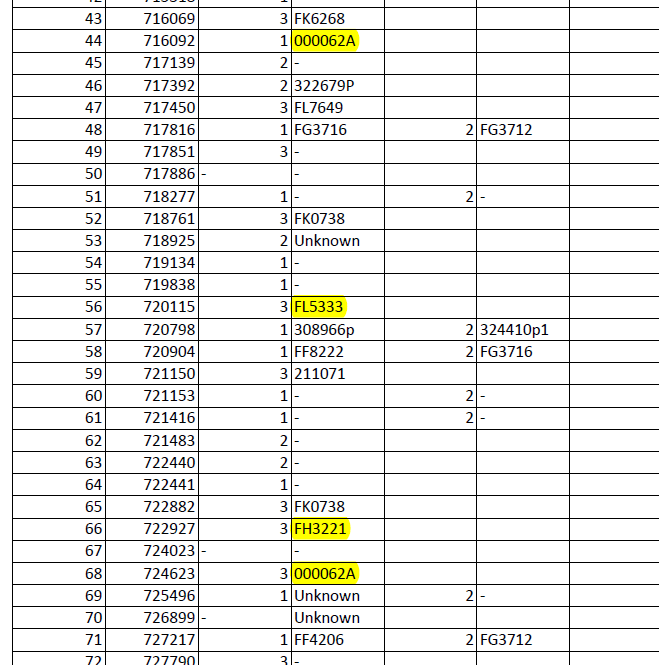
So any batch number that appears more than once is a red flag. The obvious ones are FL5333, FH3221 and 000062A.
What are the odds that those batch numbers appear in a freedom of information request put in on the 6th December 2021, which was partially rejected?
What are the odds that those batch numbers appear in a freedom of information request put in on the 6th December 2021, which was partially rejected?
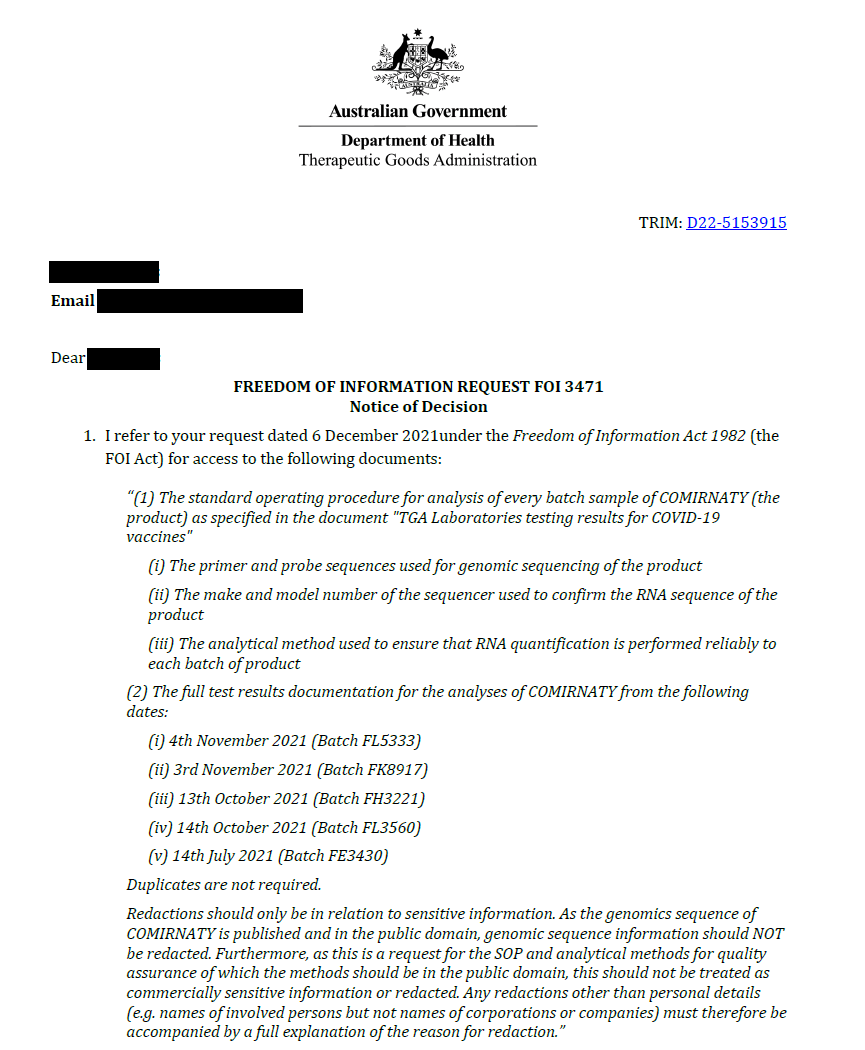
From FOI 3471 the requested primer sequences and Batch analysis of FK8917 (which no longer appears on the TGA's website) were rejected, but they did provide batch analysis of the other batches requested - of which two (of 4) appear on the "death batch" list.
What are the odds?
What are the odds?
BUT - in the 57 documents there was something that stuck out and which I posted about earlier in the year.
Because this account was suspended, that information was hidden from the public.
Because this account was suspended, that information was hidden from the public.
https://twitter.com/Jikkyleaks/status/1540939683772805121
This goes all the way back to April or before.
https://twitter.com/Jikkyleaks/status/1510925159645212674
So this is the bombshell.
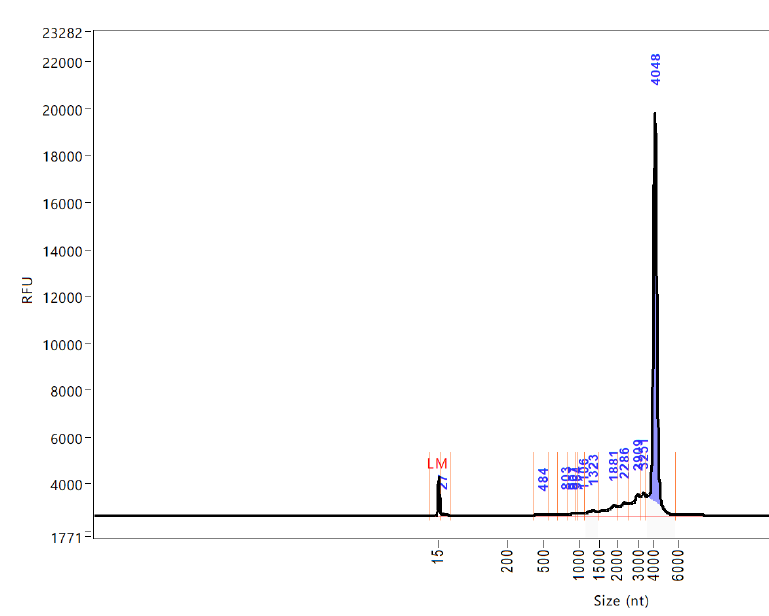
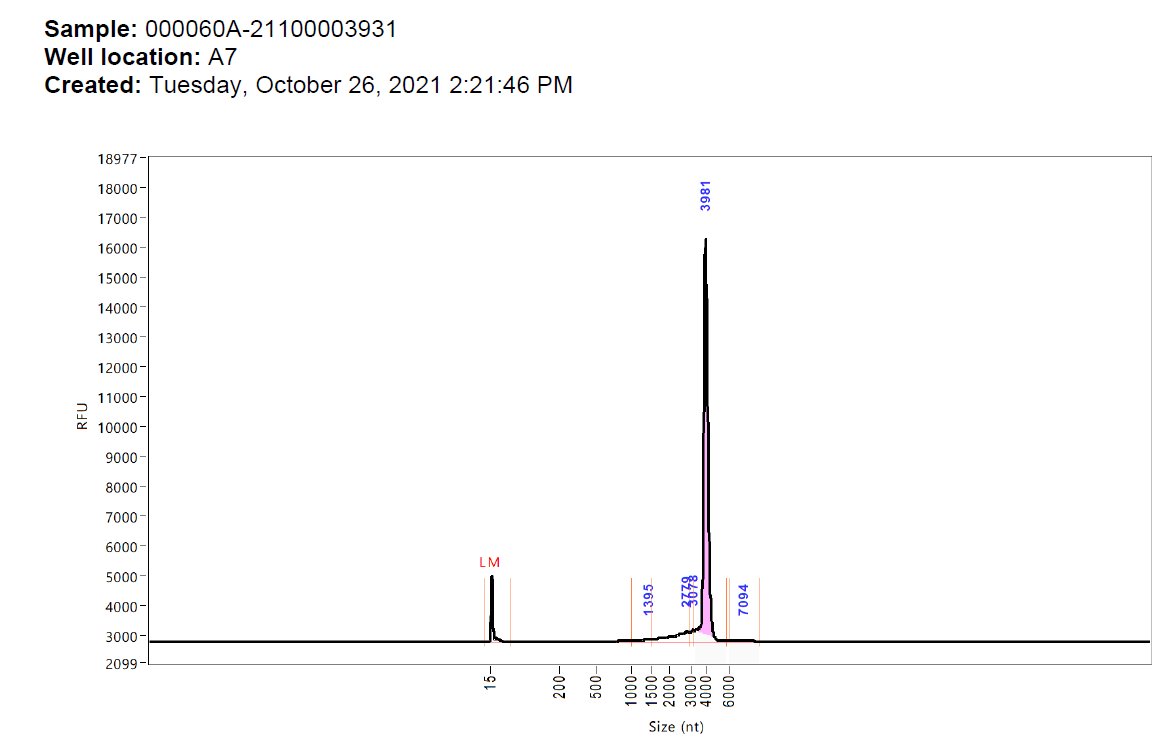
▶️The Agilent curve showed irregularities in the RNA analysis that was ignored by the TGA.
Here they are. Note the batch numbers
FL5333, FH3221, FK0738 and FL7649 - all death batches.
▶️The Agilent curve showed irregularities in the RNA analysis that was ignored by the TGA.
Here they are. Note the batch numbers
FL5333, FH3221, FK0738 and FL7649 - all death batches.
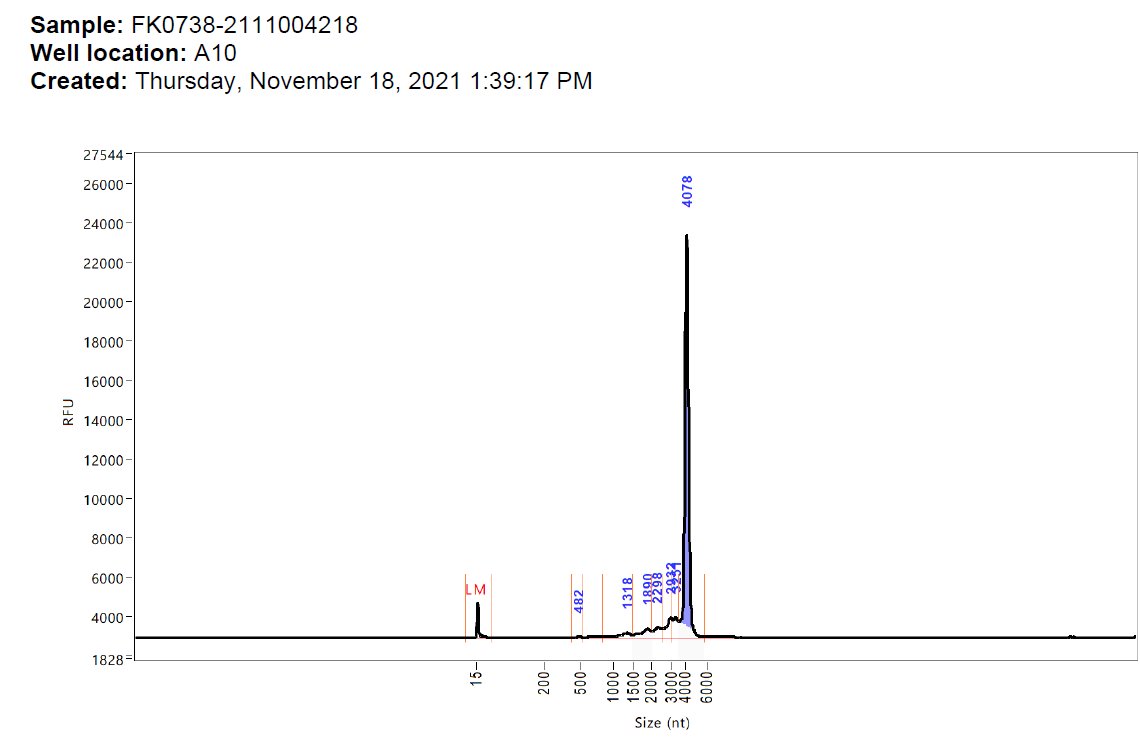
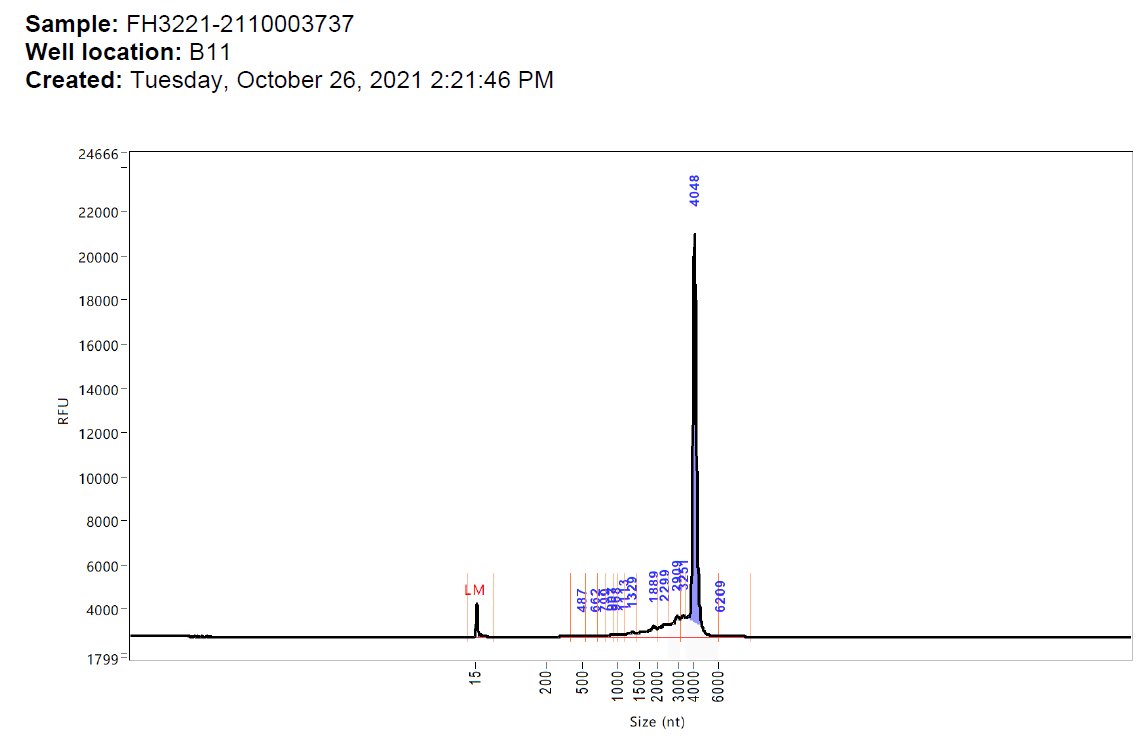
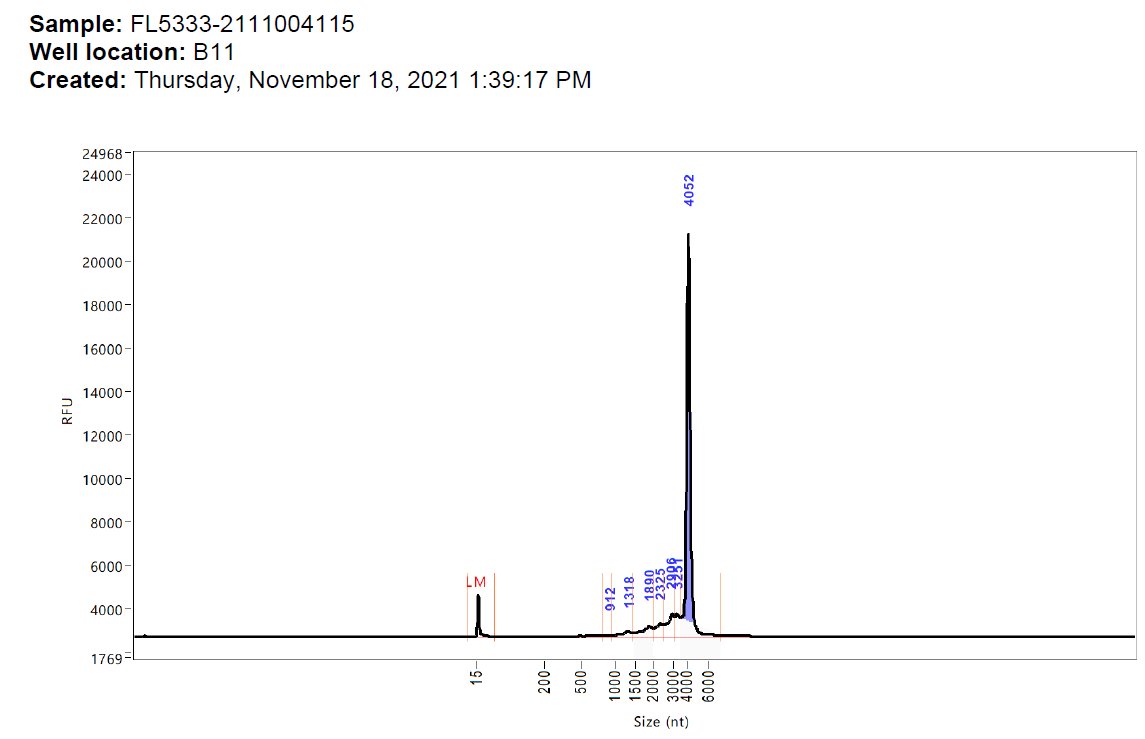
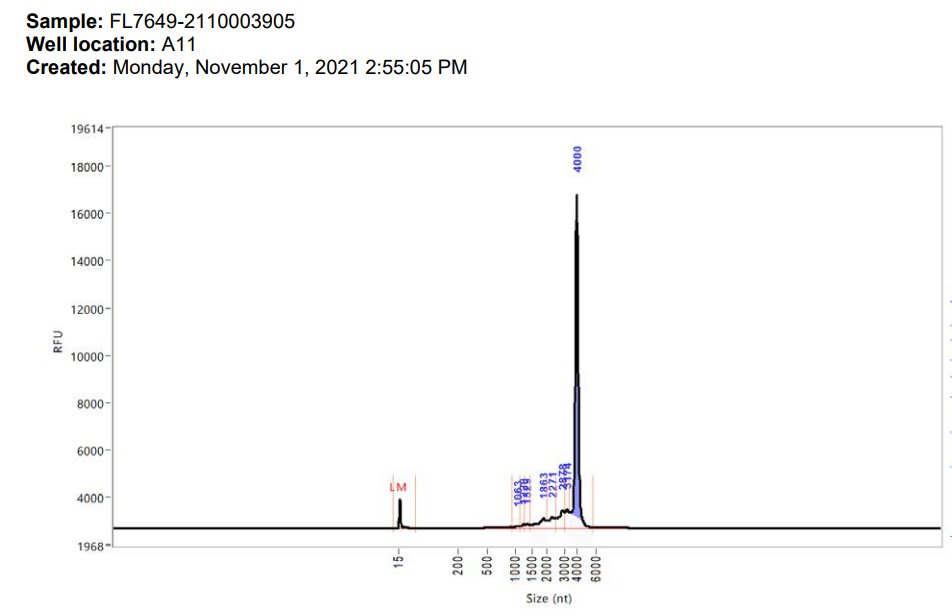
To illustrate what I'm talking about I've put a big red arrow on the point of interest. Subtle eh?
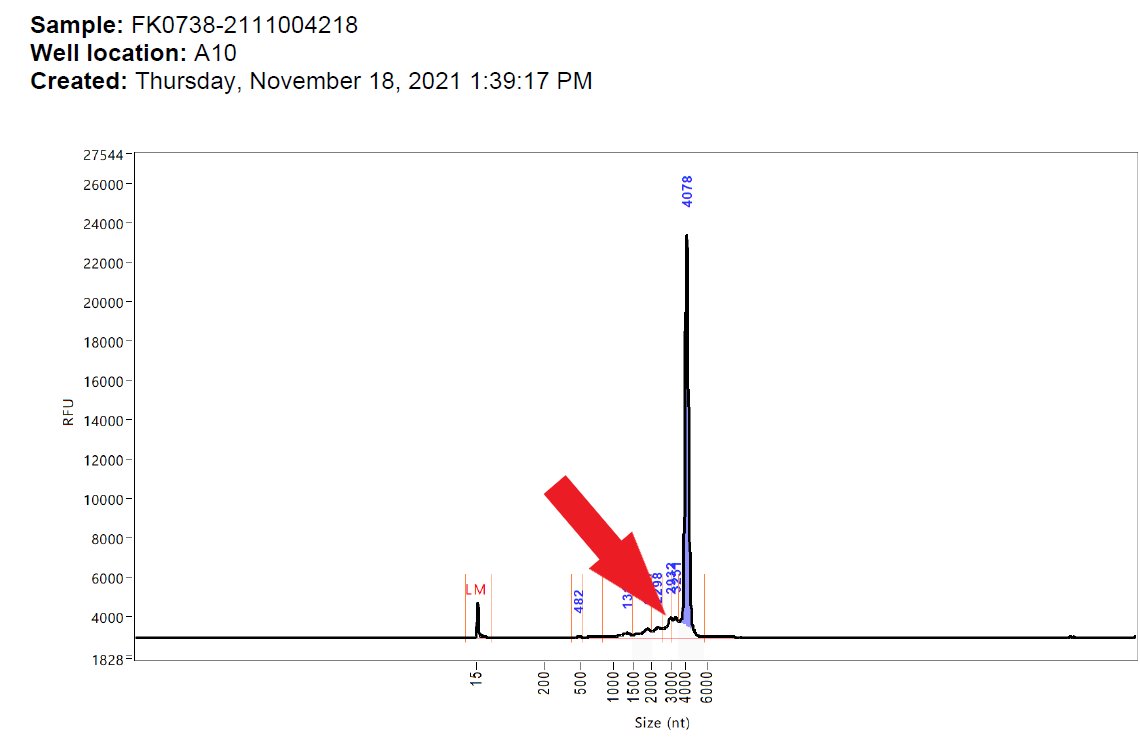
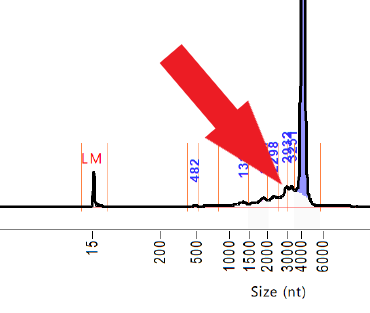
Now that hump (at about 3000nt) shouldn't be there. There is a smaller one at about 2000nt.
That agilent analysis (which should show a spike at the size of RNA of interest) shows RNA contamination.
There is RNA there that shouldn't be there
That agilent analysis (which should show a spike at the size of RNA of interest) shows RNA contamination.
There is RNA there that shouldn't be there
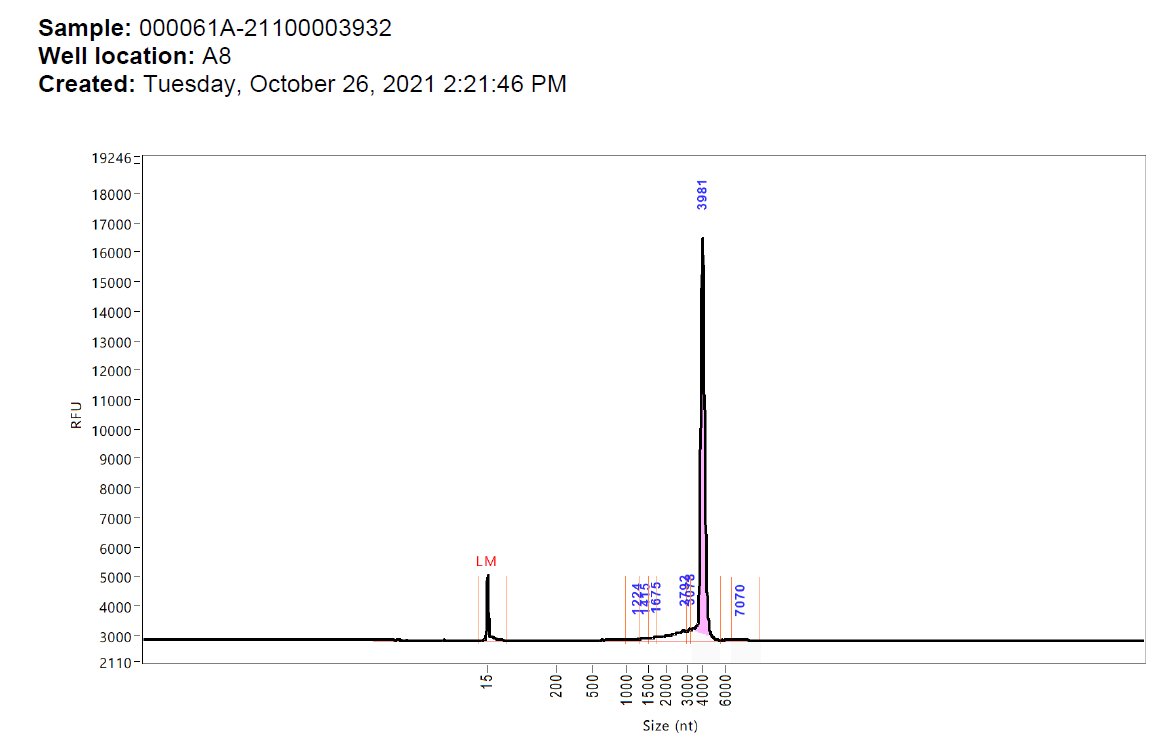
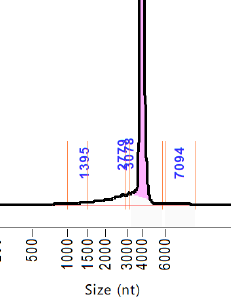
To illustrate the point further there ARE batches that don't have these humps. This is what an Agilent analysis of a relatively pure RNA should look like.
A nice smooth transition from the main spike. No humps.
These batches are not in the death log.
A nice smooth transition from the main spike. No humps.
These batches are not in the death log.
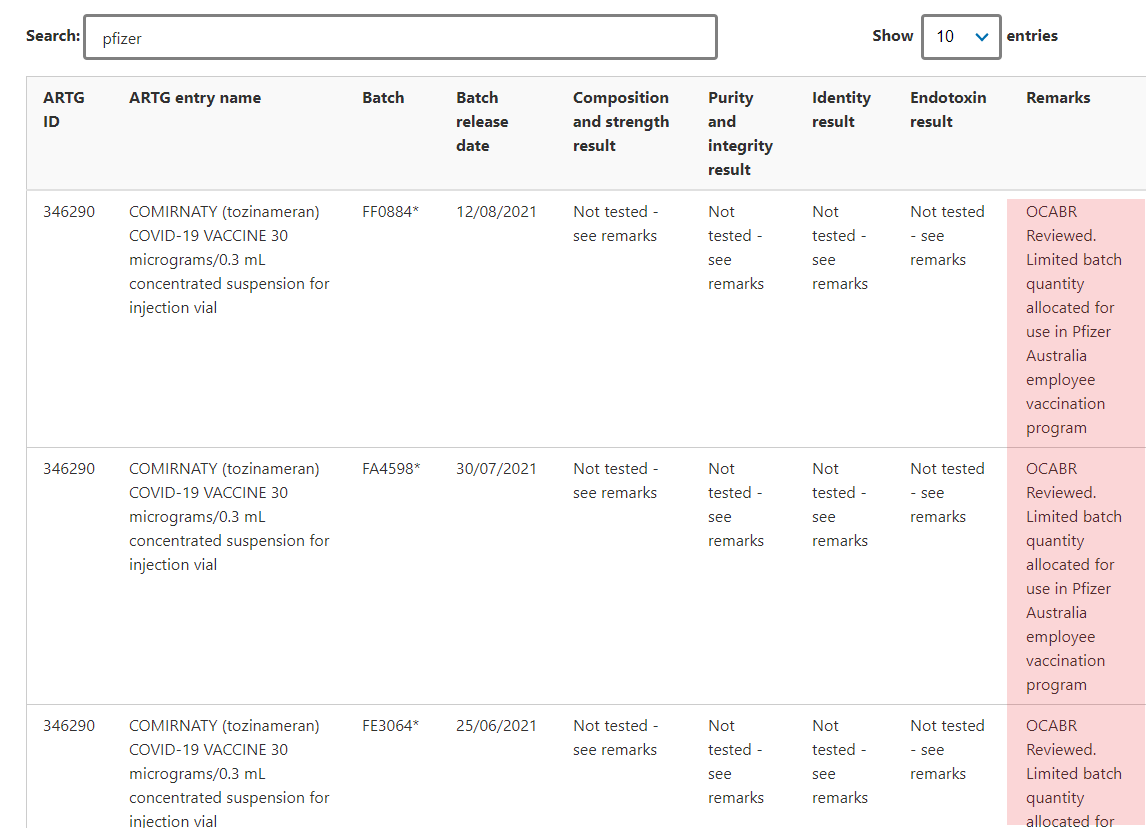
Do you know what else is not in the death batch log?
Any of the 7 batches reserved for Pfizer employees.
No, I'm not kidding:
FF0884
FA4598
FE3064
FA7338
FA7812
FC8736
FC3558
tga.gov.au/batch-release-…
Any of the 7 batches reserved for Pfizer employees.
No, I'm not kidding:
FF0884
FA4598
FE3064
FA7338
FA7812
FC8736
FC3558
tga.gov.au/batch-release-…
So, on the information that we have available (which is restricted) we must conclude that the contaminated batches lead to deaths which were not investigated and the contamination was ignored.
Of course, the TGA can tell you that they "didn't know" that these agilent curves showed contamination.
You know why?
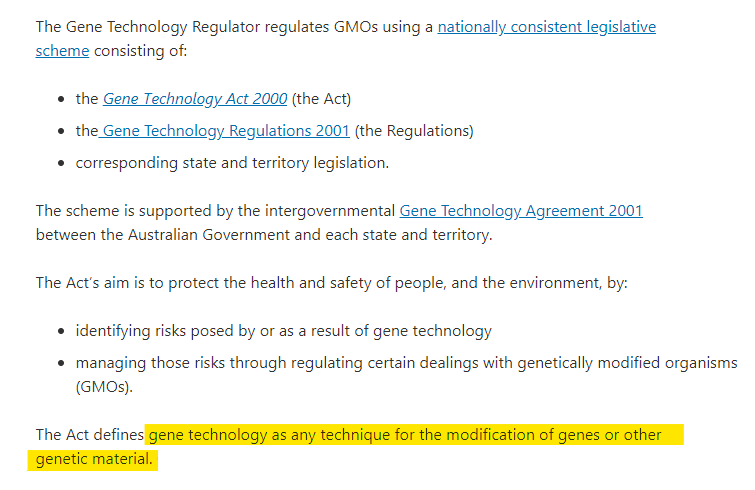
Because they didn't know how to handle genetically transferable material. The very definition that should have meant referral to the OGTR.
You know why?
Because they didn't know how to handle genetically transferable material. The very definition that should have meant referral to the OGTR.
And you know what else the TGA (and equally the FDA, MHRA and EMA) didn't know about this novel gene technlology?
Everything.
We asked them.
They had (and have) no idea what they were dealing with.
They just approved it because someone told them to.
And people died.
Everything.
We asked them.
They had (and have) no idea what they were dealing with.
They just approved it because someone told them to.
And people died.
Just a note of thanks to the helper mice that have bravely put themselves out to make these requests.
You know who you are.
You know who you are.
I should just add this extra bombshell from a few days ago here...
https://twitter.com/TheJikky/status/1606591158200963074
• • •
Missing some Tweet in this thread? You can try to
force a refresh