1/ New research shows that the type of antibody radically shifts upon the 3rd dose of mRNA. Potential implication is losing the ability to launch a viable immune response against future infections. 
2/There are four subtypes of IgG antibodies, labeled IgG1, IgG2, IgG3, and IgG4. By far, IgG1 is the predominant subclass of antibody which is present after an infection. IgG1 antibodies can neutralize an infection, and also help clear an infection.
3/In this paper, they show the normal IgG1 response after the first 2 doses, but after the third dose an unusual and sharp increase in IgG4 is observed in almost all vaccinees. An IgG4 response is not normally seen with other vaccines or repeated infections.

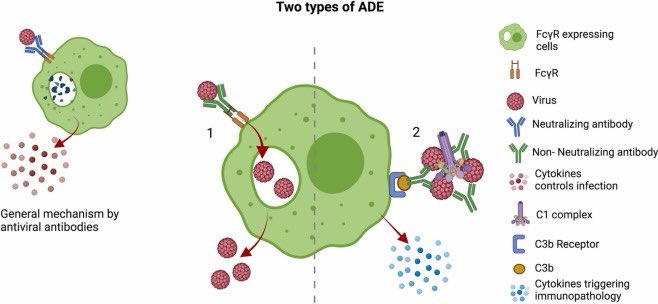
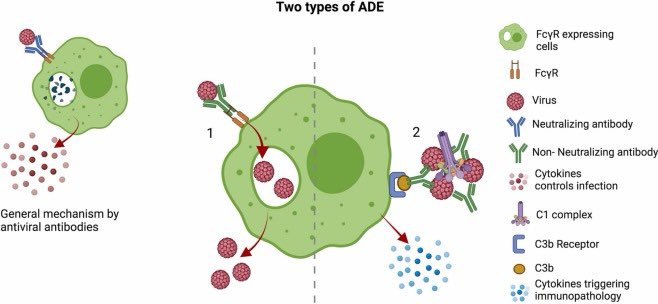
4/IgG4 is a non-inflammatory antibody, with the ability to bind and neutralize soluble or membrane bound spike protein. However, unlike IgG1 antibodies, IgG4 are terrible at launching effector functions that mobilize cellular clearance of the virus.
5/More specifically, IgG4 exhibits decreased Fc-mediated antibody effector functions including decreased antibody-dependent cellular phagocytosis (ADCP), cellular cytotoxicity (ADCC) and complement deposition (ADCD). These are required to help with viral clearance.
6/“In our study, antibody-mediated phagocytic activity and complement deposition were reduced in sera after the third immunization, in parallel to higher proportions of anti-spike IgG4 antibodies.”
7/“Since Fc-mediated effector function could be critical for viral clearance, an increase in IgG4 subclasses might result in longer viral persistence in case of infection.”
8/“However, it is also conceivable that non-inflammatory Fc-mediated effector functions reduce immunopathology while virus is still being neutralized via high-avidity antibody variable regions.”
9/“In a cohort of vaccinees with breakthrough infections, we did not obtain any evidence for an alteration of disease severity, which was mild in almost all of our cases. Larger cohorts with differential disease severities will be needed to address this aspect in the future.”
10/“Nevertheless, a Brazilian study during the early phase of the pandemic correlated an early onset and high levels of anti-spike IgG4 antibodies with a more severe COVID-19 progression after SARS-CoV-2 infection, which might indicate a less effective antibody response.”
11/“Additionally, Della-Torre et al. reported on a significant association of high IgG4/IgG1 ratios with poor disease outcome.”
12/If repeated booster doses further skew the antibody pool towards IgG4, this could translate into an impaired ability to clear future infections.
13/ Reference: science.org/doi/10.1126/sc…
14/A book you might enjoy…
https://twitter.com/sciencewdrdoug/status/1579649504722440193
• • •
Missing some Tweet in this thread? You can try to
force a refresh