Interesting published in the BMJ on long COVID from Israel. Despite EHRs known to underestimate long COVID (these should be considered the lower bound), it shows
-significant burden of symptoms in mostly young people with 'mild' COVID at 6mo-1 yr
- ⬆️in strep tonsillitis
🧵
-significant burden of symptoms in mostly young people with 'mild' COVID at 6mo-1 yr
- ⬆️in strep tonsillitis
🧵
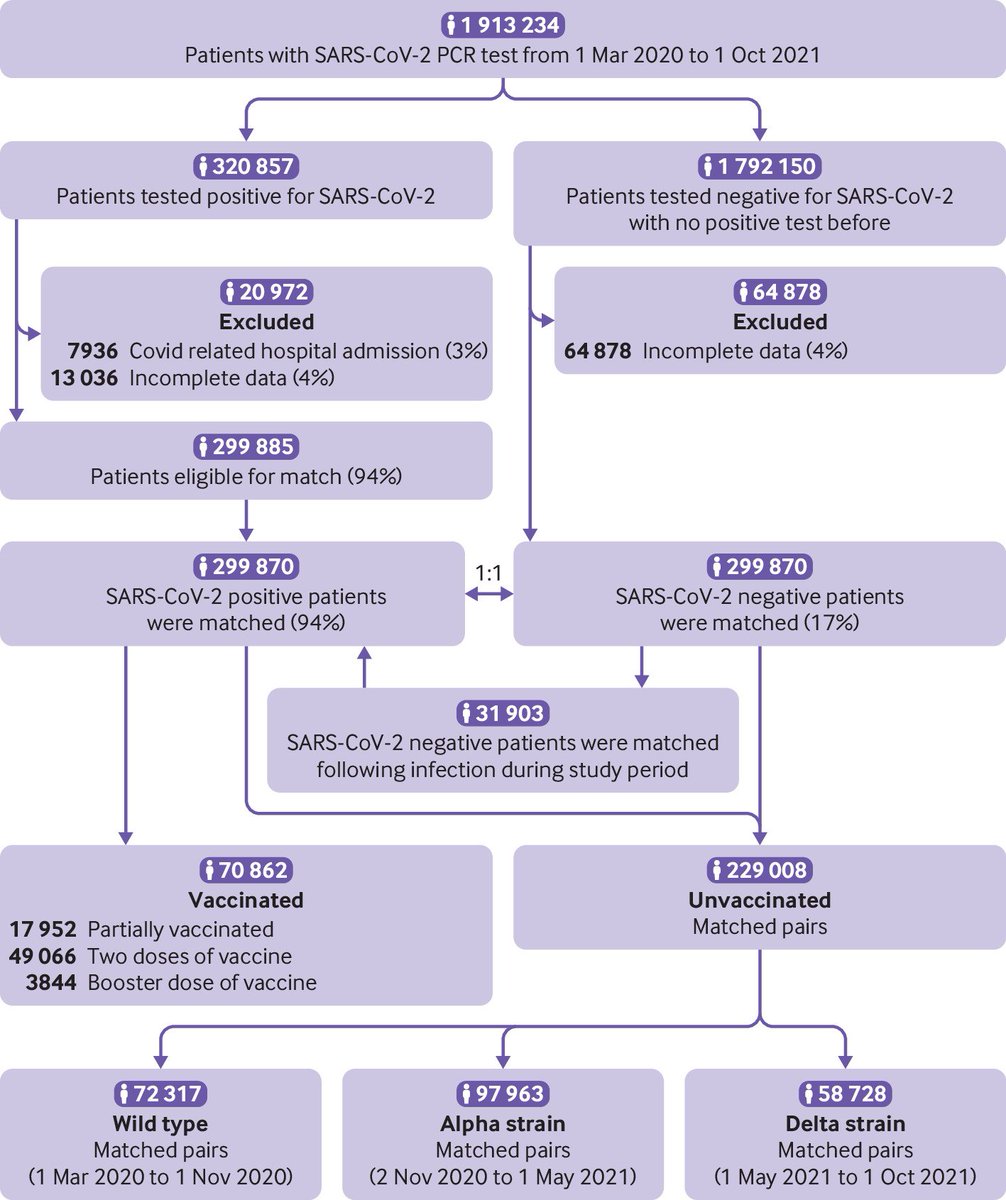
The study is a study of electronic health records from Maccabi Health services, Israel. It includes anyone who had a PCR test (+ve or -ve) between 1 March 2020 and 1 October 2021 (pre-omicron).
Important: The study excludes anyone who was hospitalised within 30 days of COVID
Important: The study excludes anyone who was hospitalised within 30 days of COVID
The purpose is specifically to look at post-covid sequelae or long COVID in those with 'mild' illness- so those not hospitalised. So long COVID prevalence is not expected to be that at population level, as we know long COVID is more common in those hosp (excluded in the study)
What did they do? They matched people with a 1st +ve PCR test with those with a 1st -ve PCR test- selecting people matched by age, sex, month of test, vax status, a propensity score that accounts for co-morbidities alcohol intake, smoking, socio-economic status & flu vax status
This would hopefully remove a lot of 'confounding' - which means make the groups as similar as possible in most respects- except the exposure being studied - SARS-CoV-2 infection.
1.9 million people had a PCR test in the study period. After removing hospitalised patients within 30 days of +ve test, & those with incomplete data, there were ~300,000 people compared in the PCR +ve and -ve group each. Comparisons in unvaxed people were carried out separately. 
What outcomes did they study?
They looked at specific diagnostic codes recorded in the health records. Only structured data was used (data entered specifically as coded by clinicians) - 'free text' - letters etc. were not used. In general, this approach will miss diagnoses.
They looked at specific diagnostic codes recorded in the health records. Only structured data was used (data entered specifically as coded by clinicians) - 'free text' - letters etc. were not used. In general, this approach will miss diagnoses.
The purpose of matching of course is to try and ensure that the underascertainment of diagnoses is similar in both groups (e.g. to avoid a scenario where in one group people are less likely to access healthcare due to other reasons).
long-COVID prevalence would almost certainly be under-ascertained with electronic health records (many people with long COVID do not report symptoms to healthcare) - but post-acute sequelae (e.g. cardiovascular, pulmonary, clotting events) may be better recorded.
Two types of events were considered: recurrent events (events that can happen more than once) - for which each date they occurred was considered, and first time events for those that only occur once - when the first time of occurrence was recorded.
Again, worth noting that generally recurrent events are not always well recorded in electronic health records. E.g. if you have loss of memory recorded at one time point, it's not necessary it'll be recorded again and again.
The cohort was a young one (median age 25), so despite the large sample size likely to be underpowered to find increases in cardiovascular events, as these are very rare even at baseline in this group. The +ve group before matching was more likely to be low socio-economic status.
What did the study show?
Despite just being a health record study, among the unvaxed there was quite an excess of loss/change of taste & smell, concentration/memory changes, weakness, breathlessness. The red boxes show late effect (6 months-1yr) and blue early effect.
Despite just being a health record study, among the unvaxed there was quite an excess of loss/change of taste & smell, concentration/memory changes, weakness, breathlessness. The red boxes show late effect (6 months-1yr) and blue early effect.
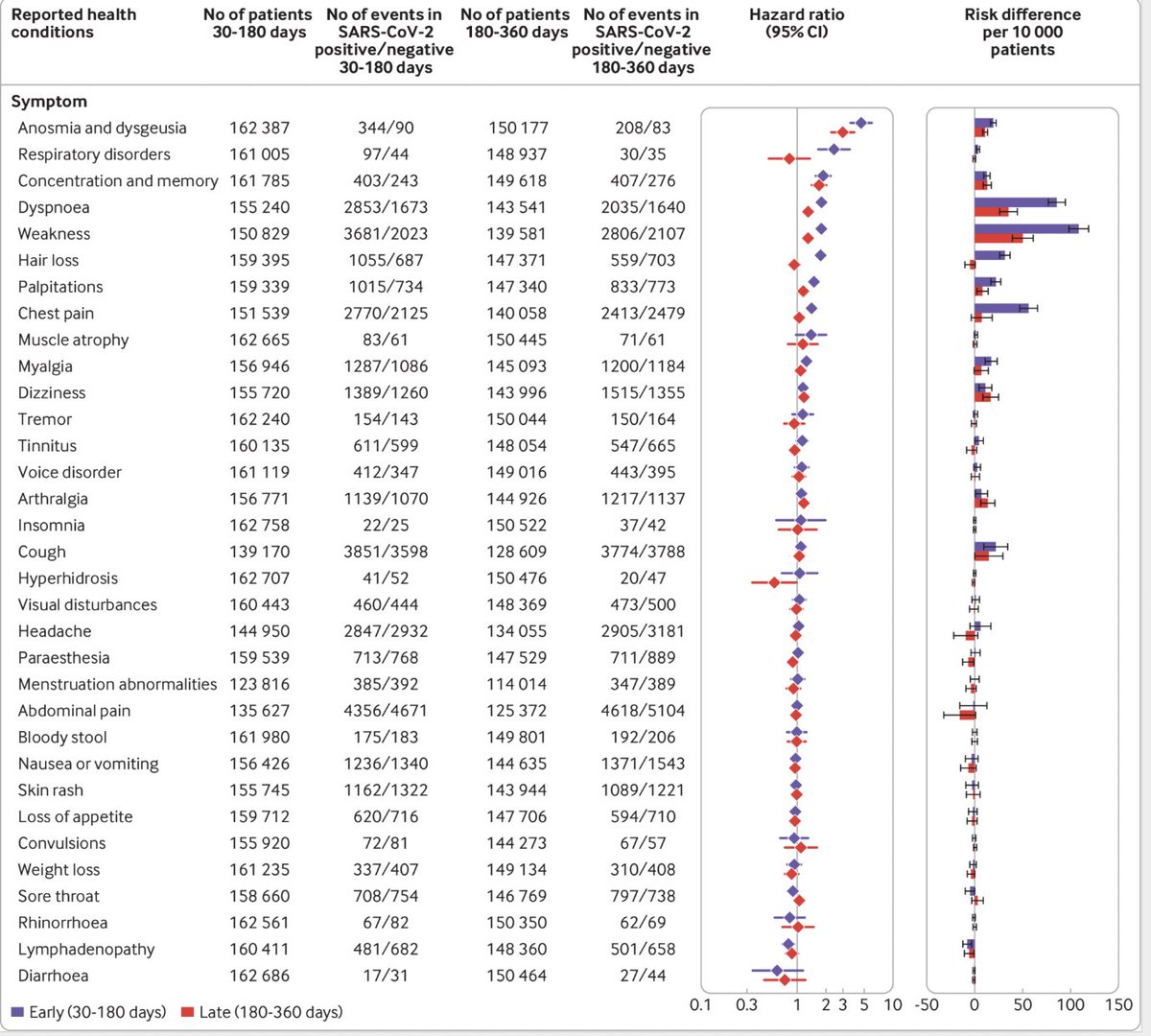
You can see that symptoms like weakness, breathlessness, change in concentration and memory, and loss of taste/smell were persistent in many, continuing 6 months-1 yr in. Memory loss particularly seemed persistent - consistent with many other studies on long COVID.
What about post-acute sequelae?
Because of the age of the population, there don't seem to have been enough events to be able to assess this- this would need larger sample sizes in such a young cohort, so hard to say much
Because of the age of the population, there don't seem to have been enough events to be able to assess this- this would need larger sample sizes in such a young cohort, so hard to say much
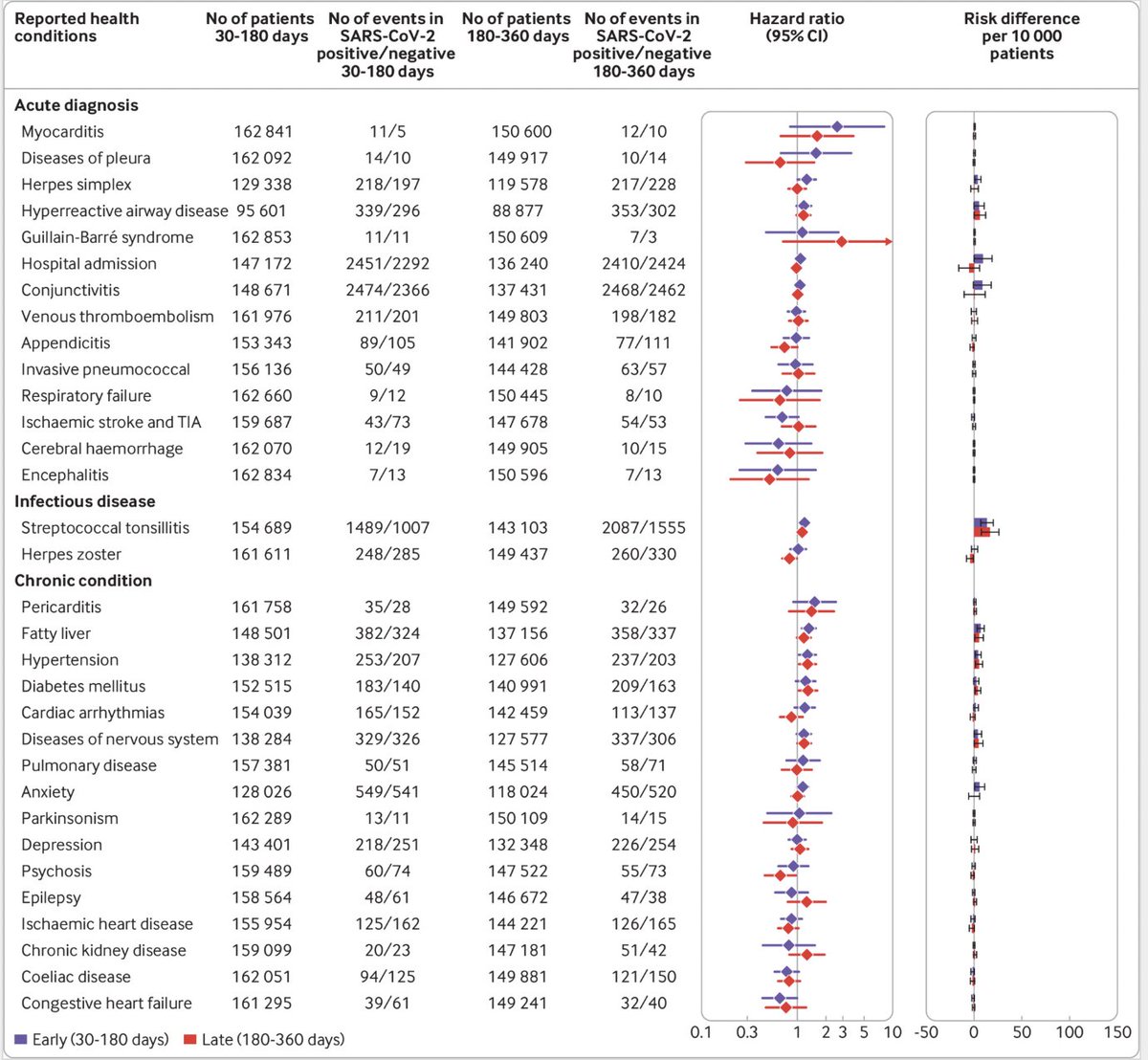
Interestingly there was a significantly excess burden of streptococcal tonsillitis-post COVID- a risk that persisted at least up to 8 months post-COVID, peaking at 6 months post-COVID. Not that these grps are adjusted for socio-economic status - so this can't explain it.
This is potentially the first observational evidence - adjusted for confounders like age, socio-economic status, co-morbidity that shows increased risk of strep infection post-COVID. Very relevant to what's being seen in the UK now in terms of serious disease with grp A strep.
The increase in risk over time for different symptoms can be visualised here. Worth remembering again that there may be underascertainment of recurrent symptoms in health records over time. So early recording may be better than late recording
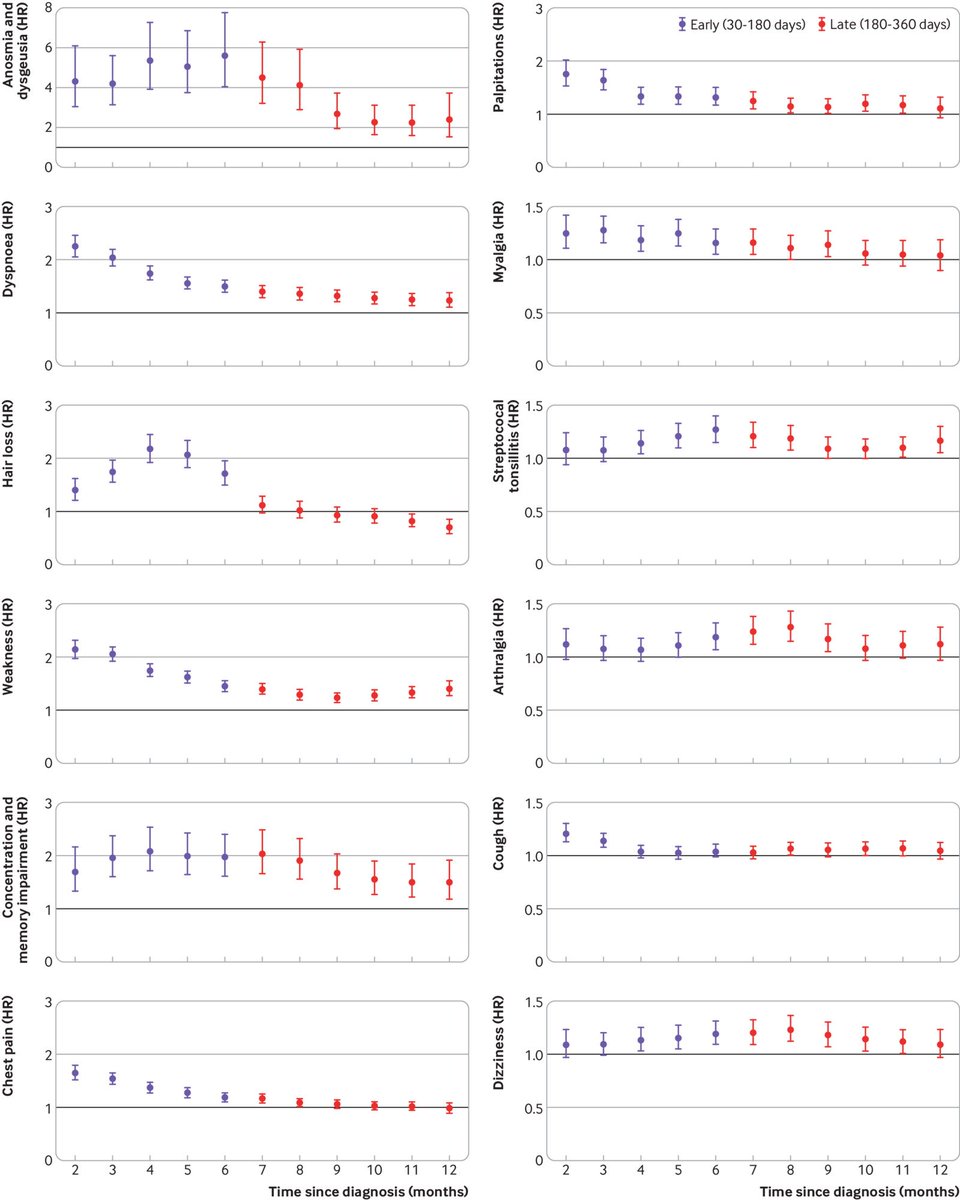
Despite this, increased risk of memory/concentration problems, weakness, breathlessness, loss of taste/smell, and dizziness persisting at 1 yr. In young people with 'mild' acute infection. Not trivial.
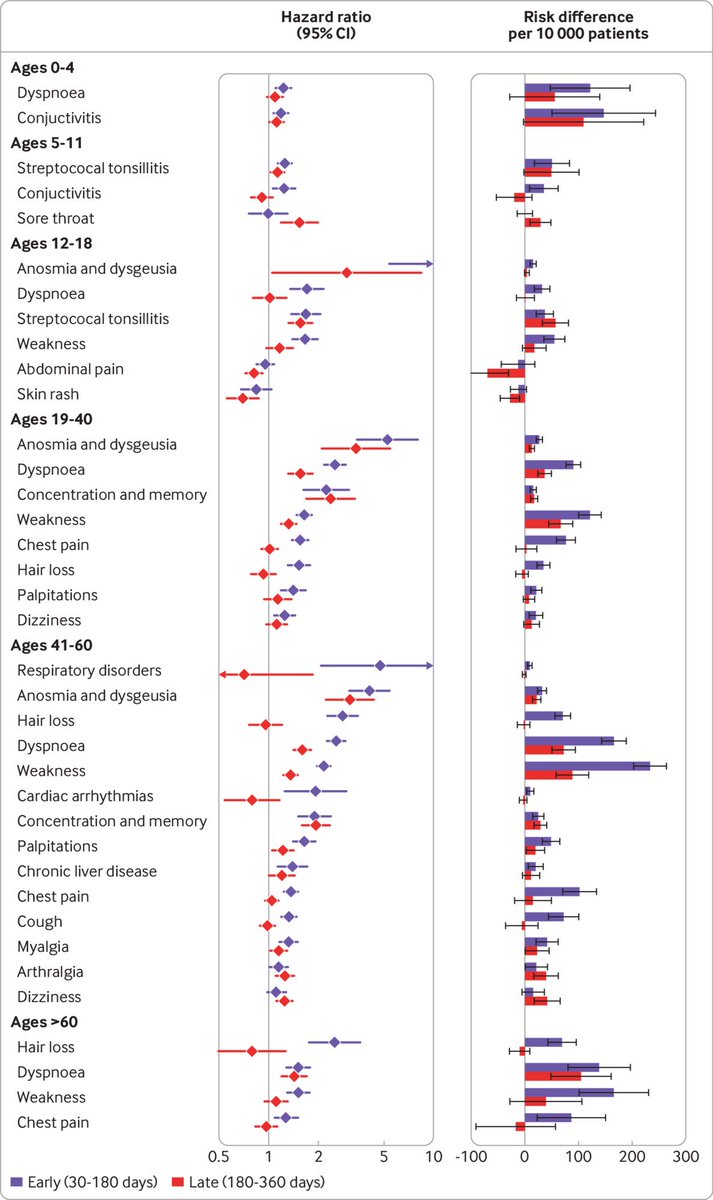
What happens when we look at it by age?
Streptococcal tonsillitis risk seems to be increased particularly in children- at least up to 1 yr post-COVID. In adults, loss of smell/taste, weakness, concentration difficulties, breathlessness are all prominent in early & late phases.
Streptococcal tonsillitis risk seems to be increased particularly in children- at least up to 1 yr post-COVID. In adults, loss of smell/taste, weakness, concentration difficulties, breathlessness are all prominent in early & late phases.
For most outcomes (except breathlessness) there was no *statistical* difference between unvaccinated and vaccinated in terms of long COVID symptom risk. The study was underpowered to detect this, so doesn't necessarily mean there is no real difference.
To summarise - this is a study only of 'mild' COVID in mostly young people - showing increased risk of several symptoms post-COVID lasting up to 1 year. The burden of these even in young people is non-trivial. Also an increased risk of post-COVID strep tonsillitis in children.
This needs to be interpreted within the limitations of the study- the primary one being that it's based on medical records which generally underascertain long COVID symptoms. And low power to look at vascular outcomes in this age group.
Study linked here:
bmj.com/content/380/bm…
And I'm hearing this study has been used to minimise long COVID in the media- the study doesn't seem to reflect the reporting though, & the authors have been quite cautious given the limitations.
bmj.com/content/380/bm…
And I'm hearing this study has been used to minimise long COVID in the media- the study doesn't seem to reflect the reporting though, & the authors have been quite cautious given the limitations.
• • •
Missing some Tweet in this thread? You can try to
force a refresh