The Examination in Coma
“the father of modern neurological surgery”
American neurosurgeon Harvey Williams Cushing (1869–1939)
#MedTwitter #neurotwitter #EndNeurophobia #tweetorials
1/
“the father of modern neurological surgery”
American neurosurgeon Harvey Williams Cushing (1869–1939)
#MedTwitter #neurotwitter #EndNeurophobia #tweetorials
1/
Definition
“a state of unarousable unresponsiveness”
Parts
a. level of consciousness
b. vital signs (BP & breathing pattern)
c. cranial nerves (fundoscopy + vision + brainstem)
d. motor & sensory
e. reflex
f. meningeal signs
2/
“a state of unarousable unresponsiveness”
Parts
a. level of consciousness
b. vital signs (BP & breathing pattern)
c. cranial nerves (fundoscopy + vision + brainstem)
d. motor & sensory
e. reflex
f. meningeal signs
2/
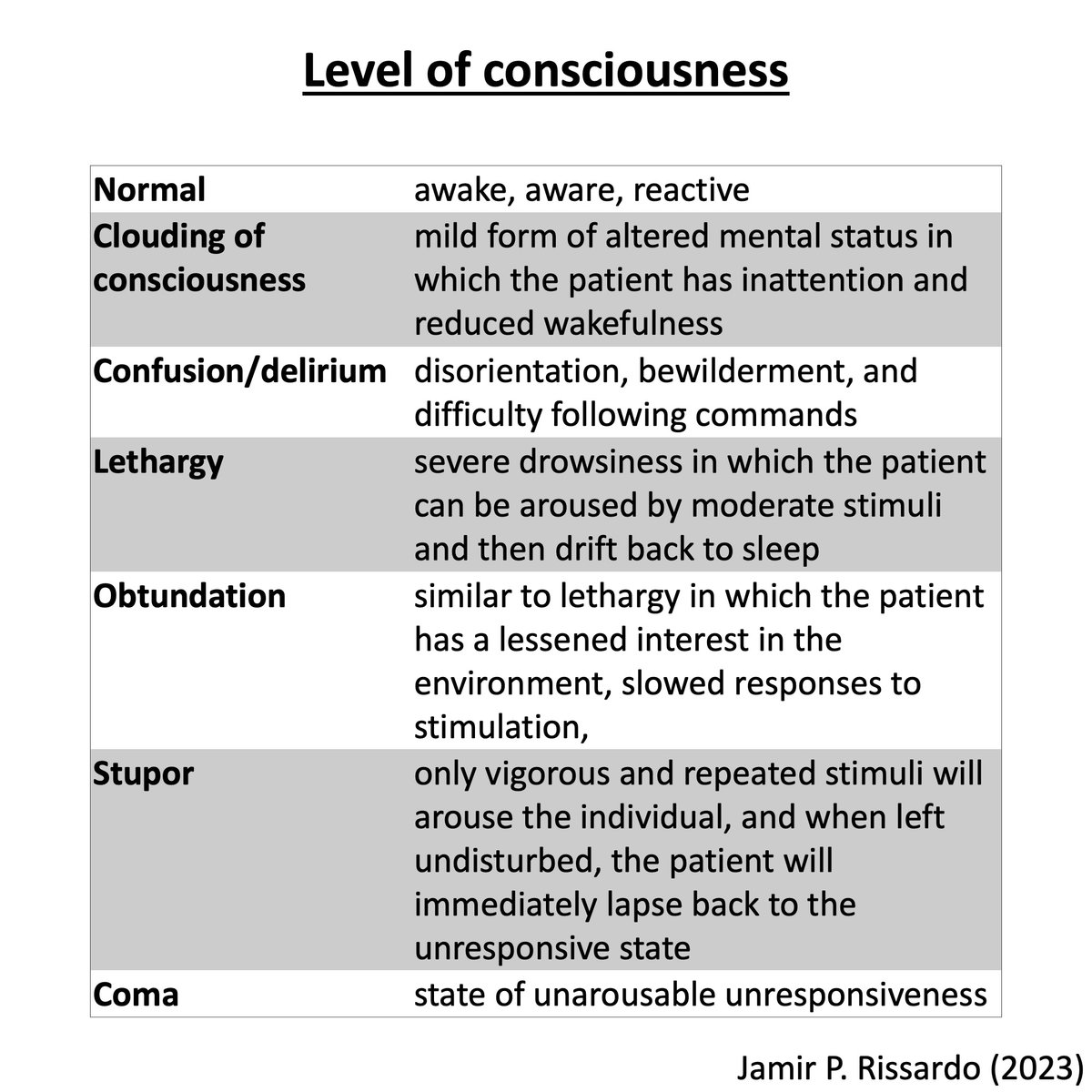
Level of consciousness
Normal
Clouding of consciousness
Confusion/delirium
Lethargy
Obtundation
Stupor
Coma
3/
Normal
Clouding of consciousness
Confusion/delirium
Lethargy
Obtundation
Stupor
Coma
3/
Grading level of consciousness
GCS (Glasgow Coma Scale)
RASS (Richmond Agitation-Sedation Score)
FOUR (Full Outline of UnResponsiveness)
4/
GCS (Glasgow Coma Scale)
RASS (Richmond Agitation-Sedation Score)
FOUR (Full Outline of UnResponsiveness)
4/
GCS (Glasgow Coma Scale)
- Parameters: best eye response, best verbal response, and best motor response
- Values between 3 and 15
- Mnemonic: EYES, VOICE, OLDBEN
5/
- Parameters: best eye response, best verbal response, and best motor response
- Values between 3 and 15
- Mnemonic: EYES, VOICE, OLDBEN
5/

RASS (Richmond Agitation-Sedation Score)
- mostly used in mechanically ventilated patients to avoid over and under-sedation
6/
- mostly used in mechanically ventilated patients to avoid over and under-sedation
6/

FOUR (Full Outline of UnResponsiveness)
- eye responses, motor responses, brainstem reflexes, and breathing pattern
7/
- eye responses, motor responses, brainstem reflexes, and breathing pattern
7/

Vital signs
a. pulse & blood pressure
- Cushing triad of increased intracranial pressure
(hypertension + bradycardia + irregular breathing)
b. breathing pattern
8/
a. pulse & blood pressure
- Cushing triad of increased intracranial pressure
(hypertension + bradycardia + irregular breathing)
b. breathing pattern
8/
Breathing pattern
“special attention to the breathing pattern, as some patterns help us localize lesions”
Breathing pattern rules
1st higher injury results in faster breathing
2nd higher injury results in more organized patterns
3rd injury to the ‘p’ons results in ‘p’auses
9/
“special attention to the breathing pattern, as some patterns help us localize lesions”
Breathing pattern rules
1st higher injury results in faster breathing
2nd higher injury results in more organized patterns
3rd injury to the ‘p’ons results in ‘p’auses
9/
Cheyne-Stokes respiration
“Hyperpnea regularly alternating w/ apnea”
- bilateral cerebral dysfunction
- increased ICP
- decreased cardiac output
via: Medical Learning Life
10/
“Hyperpnea regularly alternating w/ apnea”
- bilateral cerebral dysfunction
- increased ICP
- decreased cardiac output
via: Medical Learning Life
10/
Central neurogenic hyperventilation
“w/ respiratory alkalosis”
- damage to rostral brainstem tegmentum paramedian pontine reticular formation
- stimulation of afferent peripheral reflexes in lung and chest wall
doi.org/10.1093/med/97… via: Wijdicks
11/
“w/ respiratory alkalosis”
- damage to rostral brainstem tegmentum paramedian pontine reticular formation
- stimulation of afferent peripheral reflexes in lung and chest wall
doi.org/10.1093/med/97… via: Wijdicks
11/
Apneustic breathing
“prolonged pause at the end of inspiration”
- lateral tegmentum of the lower half of the pons
12/
“prolonged pause at the end of inspiration”
- lateral tegmentum of the lower half of the pons
12/
Cluster breathing
“periodic respirations that are irregular in frequency and amplitude with variable pauses between clusters of breath”
- lower pontine tegmental lesion
doi.org/10.1093/med/97… via: Wijdicks
13/
“periodic respirations that are irregular in frequency and amplitude with variable pauses between clusters of breath”
- lower pontine tegmental lesion
doi.org/10.1093/med/97… via: Wijdicks
13/
Ataxic breathing
“irregular in both rate and tidal volume”
- medullary damage (reticular formation of dorsomedia medulla down to obex)
14/
“irregular in both rate and tidal volume”
- medullary damage (reticular formation of dorsomedia medulla down to obex)
14/
Kussmaul breathing
“deep and labored breathing pattern”
- metabolic acidosis (diabetes ketoacidosis)
in MA, breathing is 1st rapid&shallow but as acidosis worsens, breathing gradually becomes deep&labored (this latter type is aka Kussmaul)
via: Jeff
15/
“deep and labored breathing pattern”
- metabolic acidosis (diabetes ketoacidosis)
in MA, breathing is 1st rapid&shallow but as acidosis worsens, breathing gradually becomes deep&labored (this latter type is aka Kussmaul)
via: Jeff
15/
Agonal breathing
“labored breaths, gasping, and, often, myoclonus and grunting”
- lower brainstem lesion
via: Singapore Resuscitation
16/
“labored breaths, gasping, and, often, myoclonus and grunting”
- lower brainstem lesion
via: Singapore Resuscitation
16/
Respiratory center
“Boat starts and PRASaD DIVEs”
17/
“Boat starts and PRASaD DIVEs”
17/

Cranial nerves
“fundoscopy + vision + brainstem reflexes”
Fundoscopy
a. bilateral papilledema
- high ICP
b. intraocular hemorrhage
- high ICP due to subarachnoid hemorrhage (Terson syndrome)
18/
“fundoscopy + vision + brainstem reflexes”
Fundoscopy
a. bilateral papilledema
- high ICP
b. intraocular hemorrhage
- high ICP due to subarachnoid hemorrhage (Terson syndrome)
18/

Vision and eye movements
Vision
- blink-to-threat
Eye movements
- ocular bobbing
- ping-pong
- forced downward gaze
- rapid VOR w/ downward movement
- ocular myoclonus
19/
Vision
- blink-to-threat
Eye movements
- ocular bobbing
- ping-pong
- forced downward gaze
- rapid VOR w/ downward movement
- ocular myoclonus
19/
Brainstem reflexes
Brainstem Reflexes Assessment Sedation Scale (BRASS)
i. cough reflex
ii. pupillary light reflex
iii. corneal reflex
iv. absence of grimacing and absence of oculocephalic
v. absence of grimacing and presence of oculocephalic
20/
Brainstem Reflexes Assessment Sedation Scale (BRASS)
i. cough reflex
ii. pupillary light reflex
iii. corneal reflex
iv. absence of grimacing and absence of oculocephalic
v. absence of grimacing and presence of oculocephalic
20/

Pupil size
Small & reactive: metabolic and diencephalic
Large & fixed & hippus: pretectal
Dilate & fixed (unil): III nerve (uncal)
- Kernohan notch
Midposition & fixed: midbrain
Pinpoint: pons
21/
Small & reactive: metabolic and diencephalic
Large & fixed & hippus: pretectal
Dilate & fixed (unil): III nerve (uncal)
- Kernohan notch
Midposition & fixed: midbrain
Pinpoint: pons
21/

Motor & sensory exam
a. can the patient localize to painful stimuli?
- defend, localize, withdraw, flex, extend, no response
via: jamieskaff
22/
a. can the patient localize to painful stimuli?
- defend, localize, withdraw, flex, extend, no response
via: jamieskaff
22/
b. movements in coma
- arc de cercle
- choreiform fidgets
- myoclonus status epilepticus
- spontaneous triple flexion responses
23/
- arc de cercle
- choreiform fidgets
- myoclonus status epilepticus
- spontaneous triple flexion responses
23/
c. posturing
decerebrate and decorticate
24/
decerebrate and decorticate
24/

Reflexes
“the same as in the conscious person”
- muscle tone
- reflexes
- clonus
- plantar response
25/
“the same as in the conscious person”
- muscle tone
- reflexes
- clonus
- plantar response
25/
Meningeal signs
a. Nuchal (cervical) rigidity
b. Kernig's sign
c. Brudzinski's neck sign
d. Brudzinski's contralateral reflex sign
e. Tripod or Amoss's or Hoyne's sign
f. Others
26/
a. Nuchal (cervical) rigidity
b. Kernig's sign
c. Brudzinski's neck sign
d. Brudzinski's contralateral reflex sign
e. Tripod or Amoss's or Hoyne's sign
f. Others
26/
Differential
1.Coma w/ focal or lateralizing signs
- CVA (ischemic or hemorrhagic)
- Trauma
- Space occupying lesion (tumor or infectious)
2.Coma w/ meningismus
- Meningoencephalitis
- Subarachnoid hemorrhage
3.Coma w/o localizing signs or meningismus
- TOMES mnemonic
27/
1.Coma w/ focal or lateralizing signs
- CVA (ischemic or hemorrhagic)
- Trauma
- Space occupying lesion (tumor or infectious)
2.Coma w/ meningismus
- Meningoencephalitis
- Subarachnoid hemorrhage
3.Coma w/o localizing signs or meningismus
- TOMES mnemonic
27/

Coma mimicking
a. locked-in syndrome (video)
- vertical eye movements and blinking are usually spared
- awake
b. abulia & akinetic mutism
- profound failure of executive function
doi.org/10.1093/med/97… via: Wijdicks
28/
a. locked-in syndrome (video)
- vertical eye movements and blinking are usually spared
- awake
b. abulia & akinetic mutism
- profound failure of executive function
doi.org/10.1093/med/97… via: Wijdicks
28/
c. hypokinetic catatonia
- obtundation
- immobility, mutism, staring, cataplexy
- Bush-Francis Catatonia Rating Scale
d. functional unresponsiveness
- open the eyelids (tightly shut eyelids; eye movements; rapid eyelid closure)
- oculocephalic reflex
- optokinetic nystagmus
29/
- obtundation
- immobility, mutism, staring, cataplexy
- Bush-Francis Catatonia Rating Scale
d. functional unresponsiveness
- open the eyelids (tightly shut eyelids; eye movements; rapid eyelid closure)
- oculocephalic reflex
- optokinetic nystagmus
29/

NeuroTeach - Content
The blog contains all the threads and videos.
neuronland.blogspot.com/2022/11/neurot…
Have a great day!
The blog contains all the threads and videos.
neuronland.blogspot.com/2022/11/neurot…
Have a great day!
• • •
Missing some Tweet in this thread? You can try to
force a refresh