
Belangrijk rapport deze week, opmerkelijk weinig aandacht. Onderzoek oversterfte, stap 1: CBS en RIVM doen versneld de analysis die ze altijd al deden over oversterfte. Dit is gericht op oversterfte vanwege COVID over 2020 en 2021 rivm.nl/documenten/ein…
daarna volgt onderzoek naar niet verklaarde oversterfte. Hiervoor heeft ZON MW calls uitgezet. zonmw.nl/nl/over-zonmw/…
Het CBS heeft de oversterfte en sterfte aan COVID-19 en andere doodsoorzaken in 2020 en 2021 beschreven. Hierbij is gekeken naar verschillen in sterfte naar leeftijd en bij gebruik van langdurige zorg.
de eerste twee golven liepen samen op met covid pieken. de derde golf gaf een verschuiving naar ouderen en moet verder worden onderzocht 
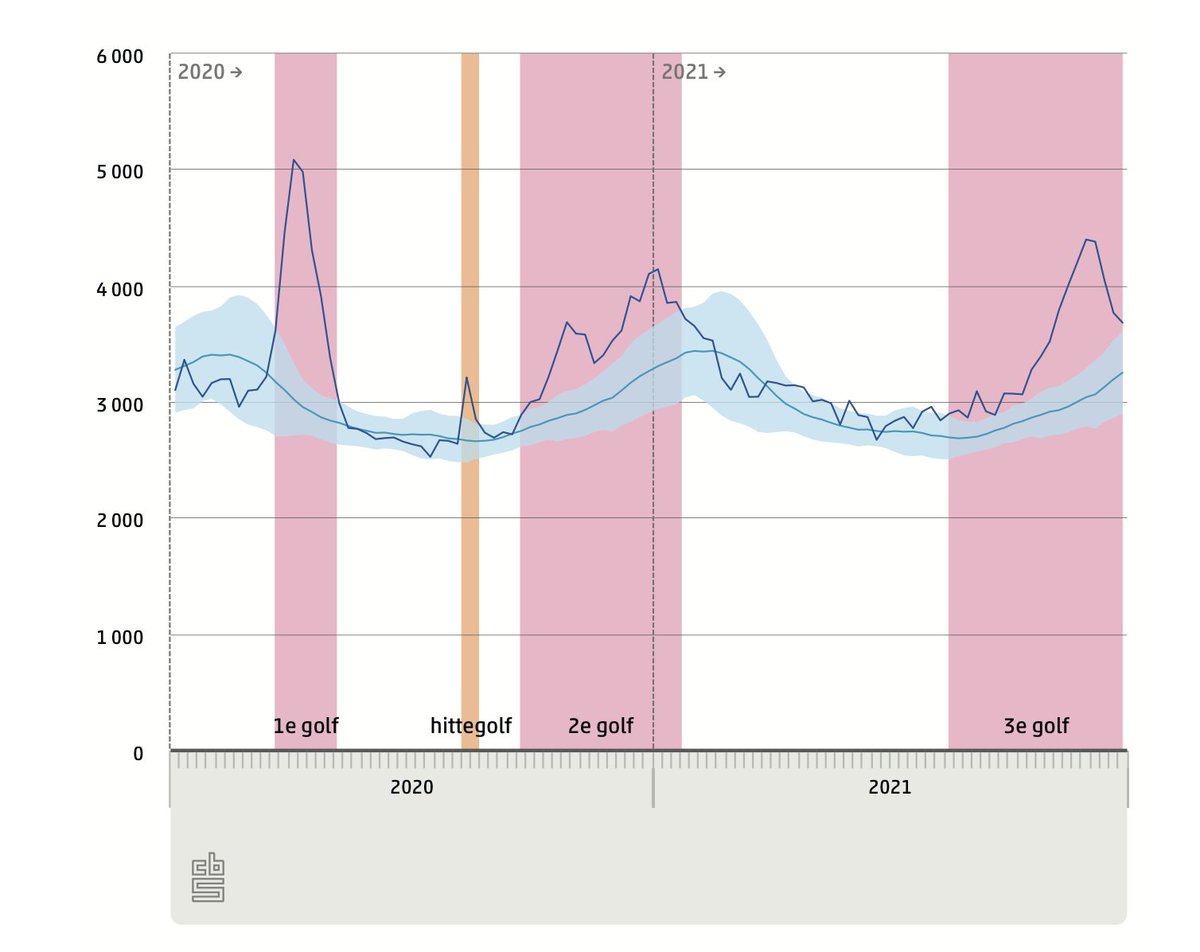
in 2020 en 2021 overleden naar schatting 30.000 mensen meer dan verwacht dan zonder covid. In totaal wordt circa 40.000 overlijdens direct aan covid toegeschreven.
in de langdurige zorg is ook een oversterfte piek te zine bij de hittegolf in die periode. Dat is een bekend fenomeen.
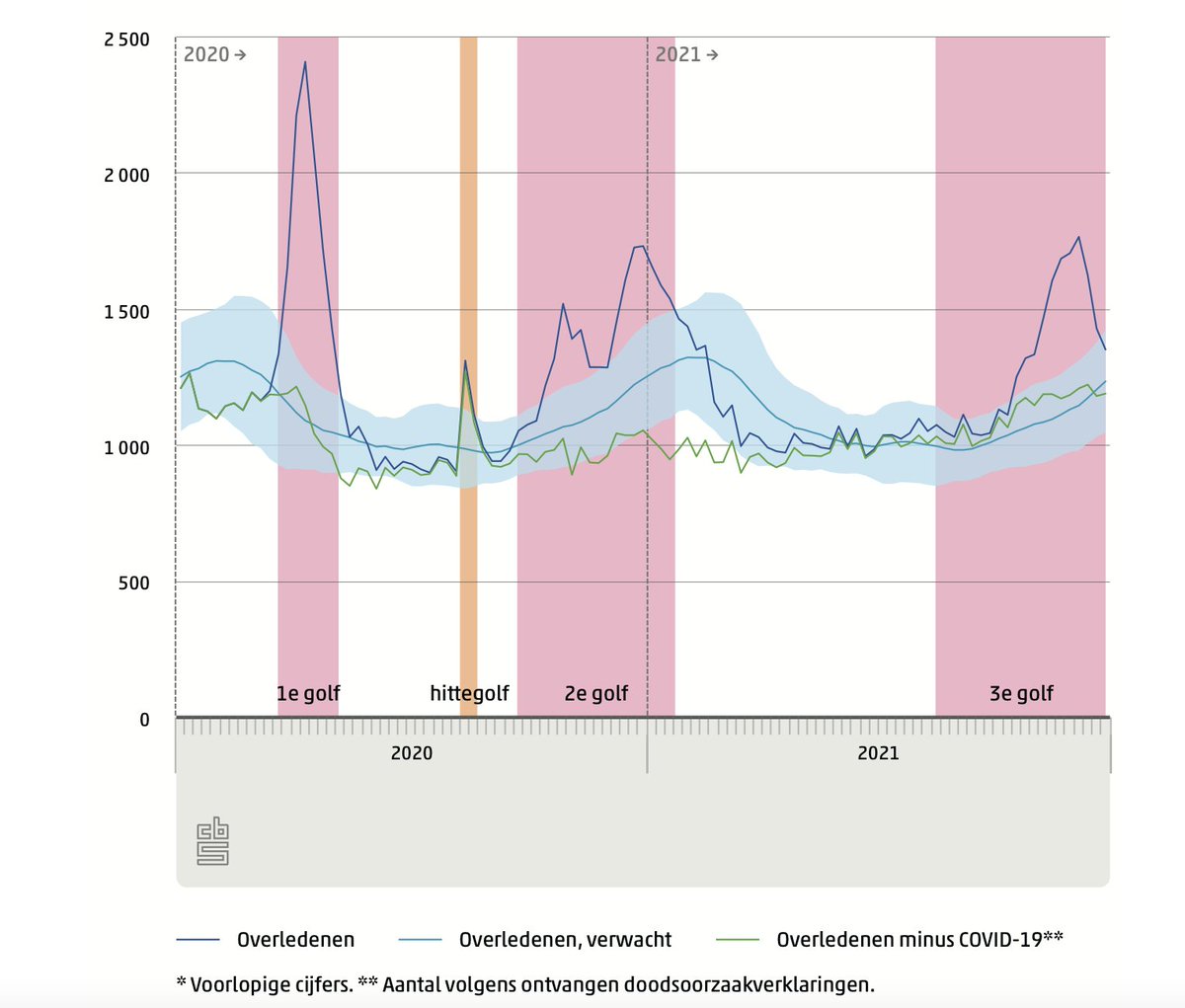
het rapport bekijkt ook het aandeel covid in het totale overzicht van doodsoorzaken

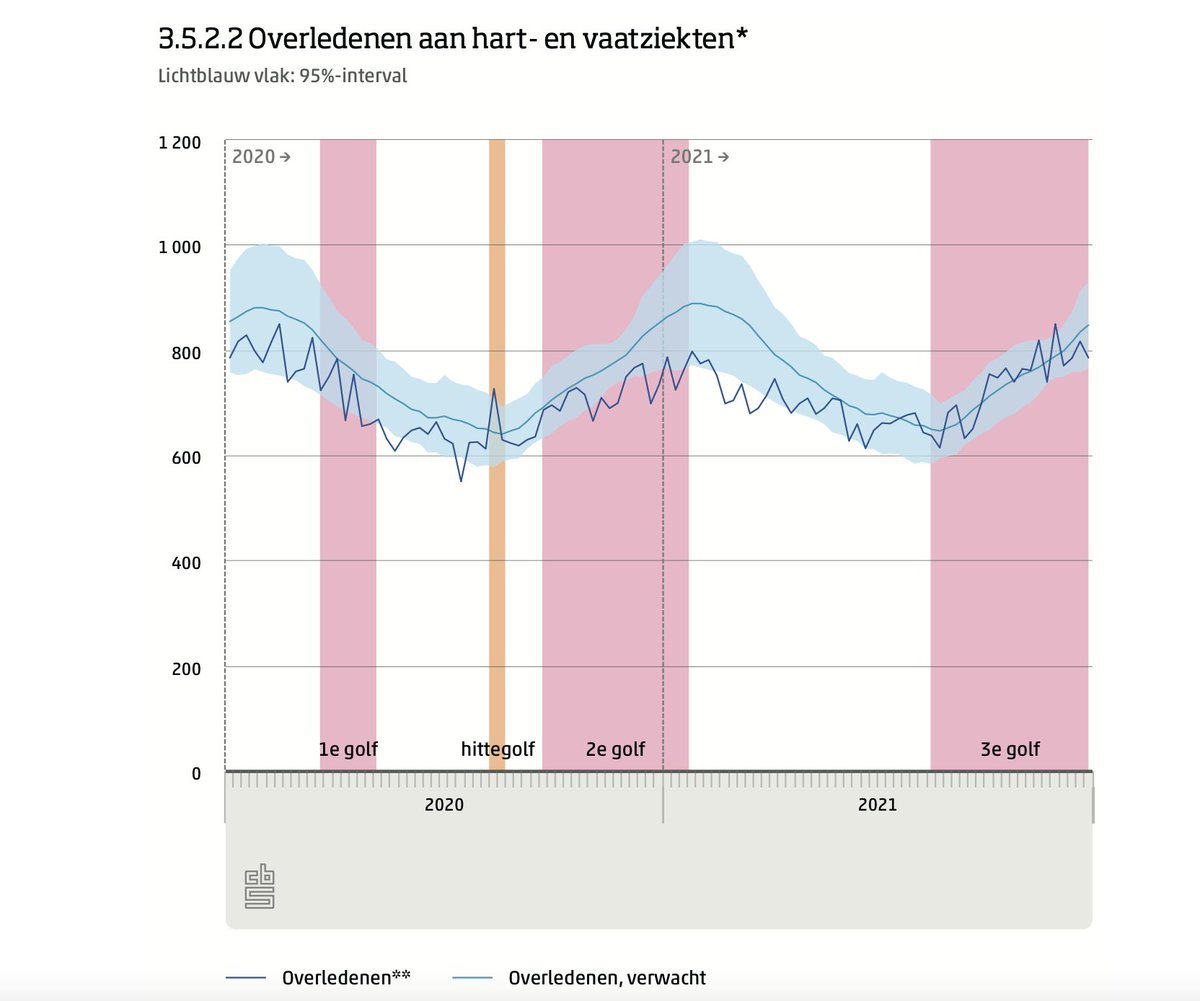
het rapport bevat interessante tussen analyses. Bijvoorbeeld trends in overlijdens aan hart en vaatziekten: iets lager dan verwacht
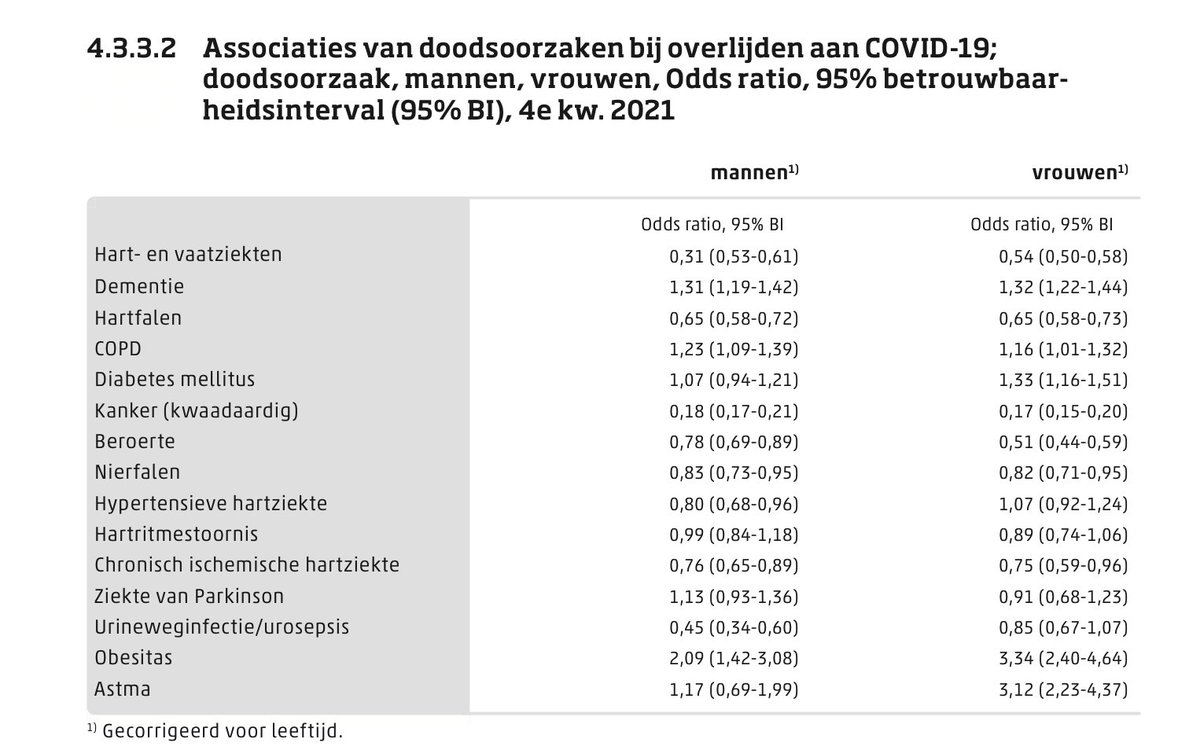
Ook de oversterfte analyses door RIVM staan in het rapport. Daar een interessante aanvulling: welke andere ziektes komen vaker voor bij mensen met COVID. Zegt wat over risicofactoren. Ik vind her wat verschillen tussen mannen en vrouwen opmerkelijk.
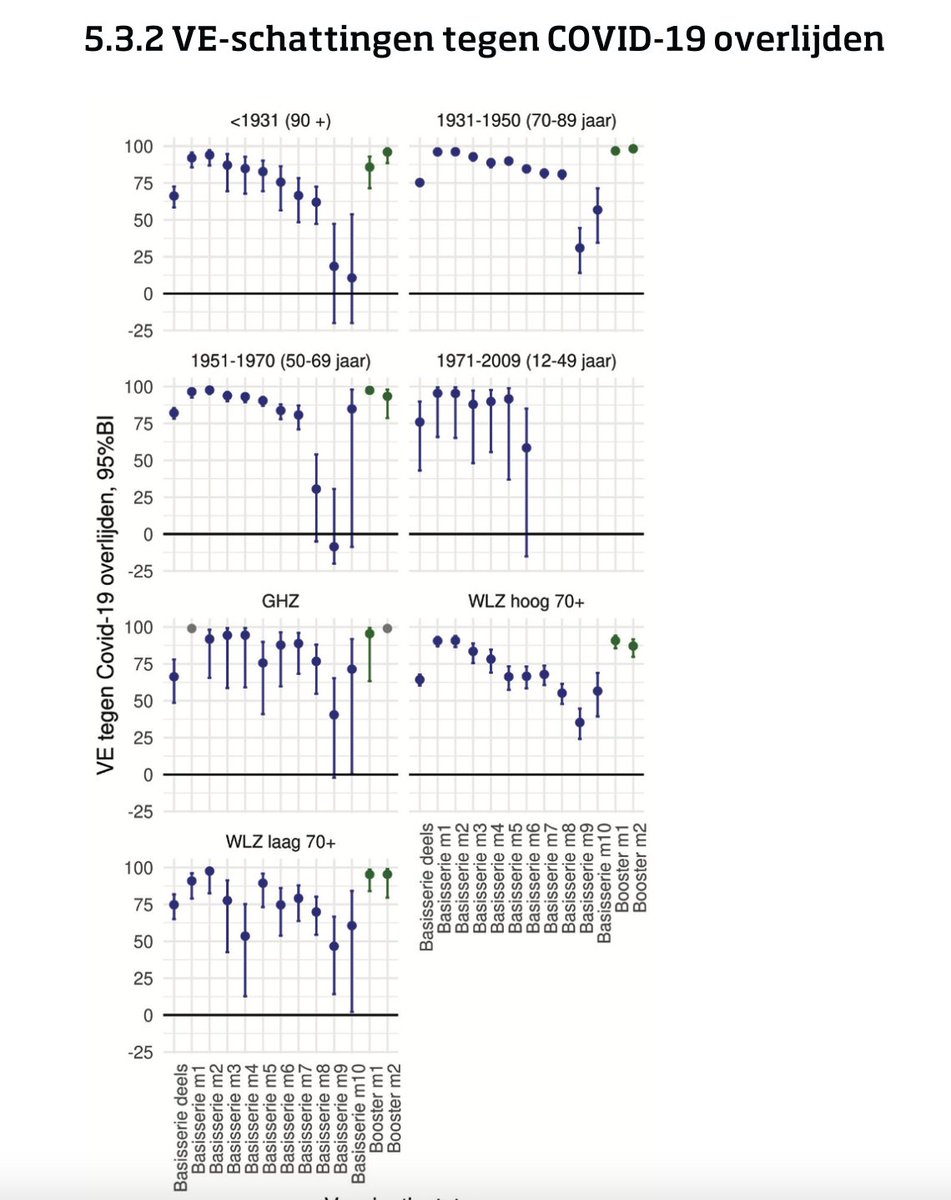
Dan, natuurlijk heel belangrijk: de mate van bescherming van vaccins tegen overlijden. NB dit is in 2021
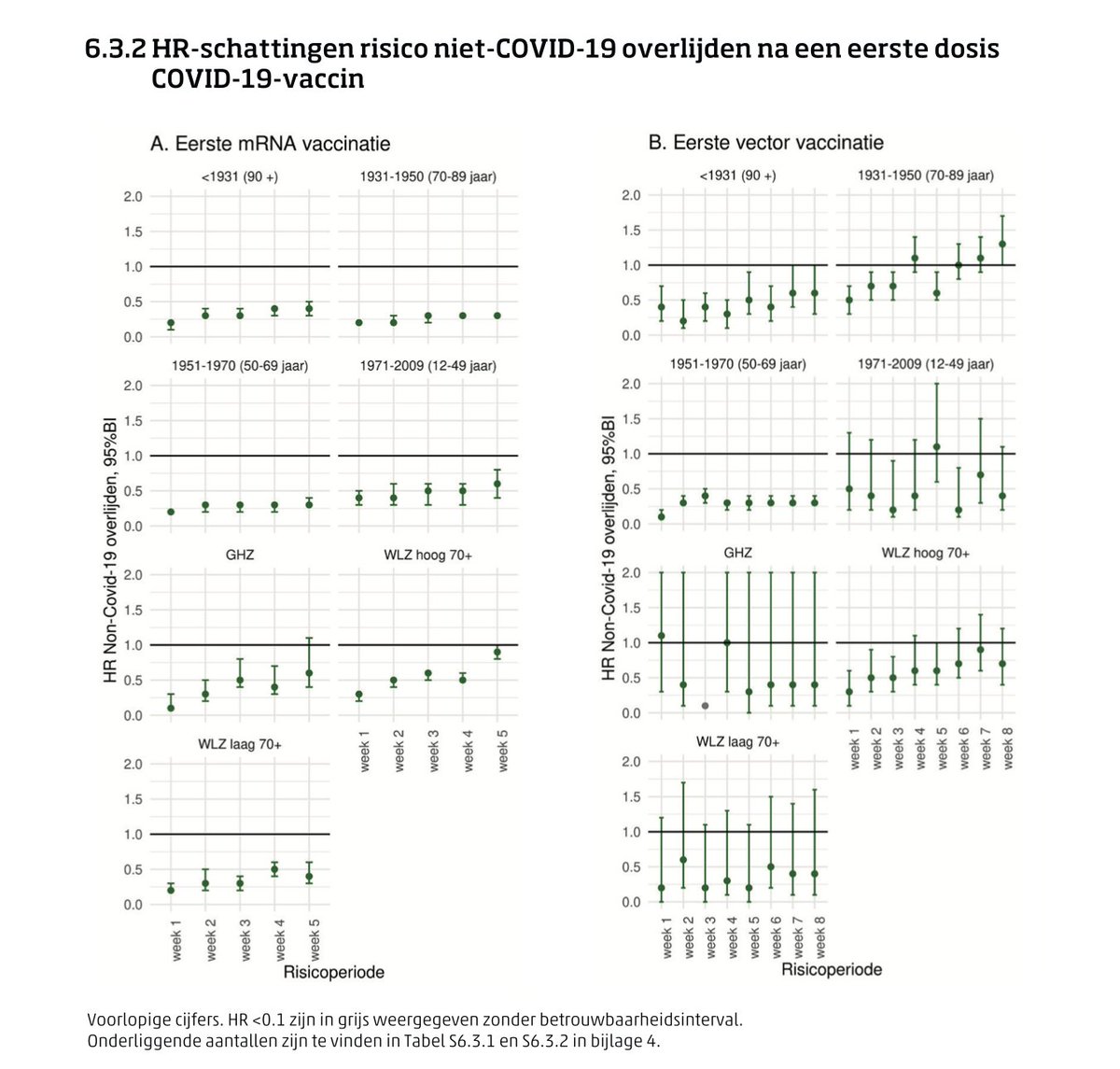
en last but not least: oversterfte kort na vaccinatie. Conclusie: die is er niet.
tenslotte een stevige conclusie: Op basis van de ervaringen in dit traject en ... in de beleidsmonitoring COVID-19, achten veel bronhouders de huidige juridische kaders niet voldoende om een optimale data-infrastructuur mogelijk te maken voor onderzoek naar COVID-19. Hearhear
correctie, was al wat ouder...
• • •
Missing some Tweet in this thread? You can try to
force a refresh



