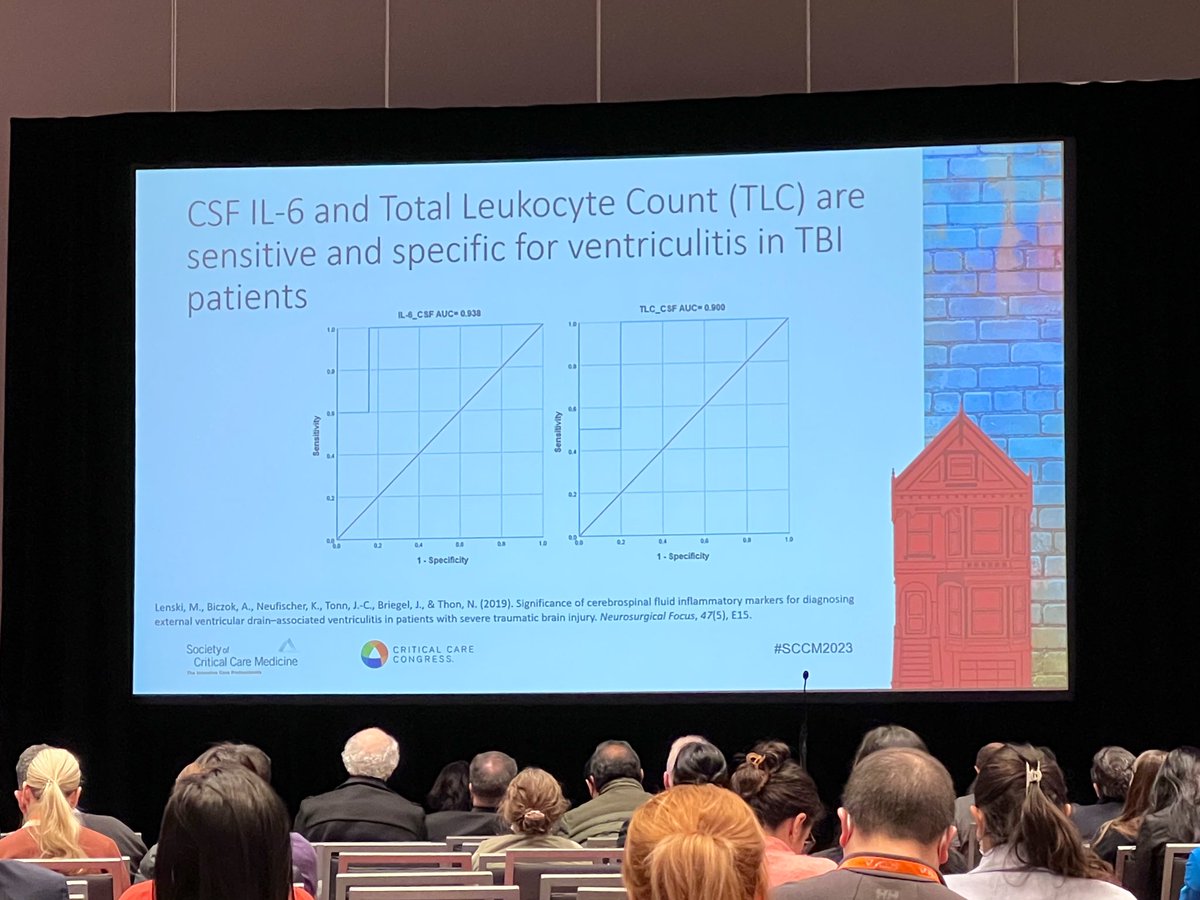
Rapid diagnostics may provide faster time to targeted therapy in HAP/VAP infections. Specificity can be as high as 99% with sensitivity to 100% in either BAL or sputum cultures.
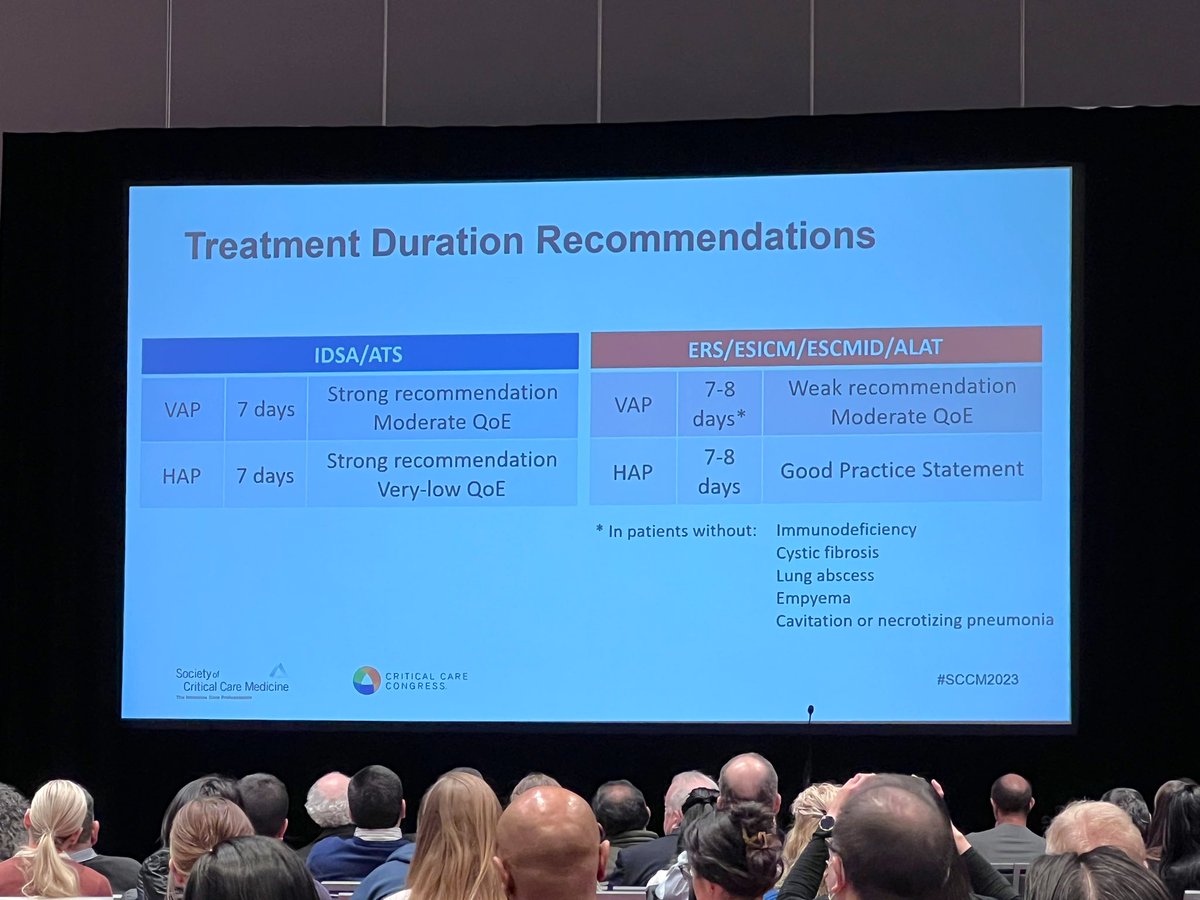
@ScottMicek reviews updates to HAP/VAP therapy and the impacts on stewardship #SCCM2023 @SCCM_CPP
@ScottMicek reviews updates to HAP/VAP therapy and the impacts on stewardship #SCCM2023 @SCCM_CPP

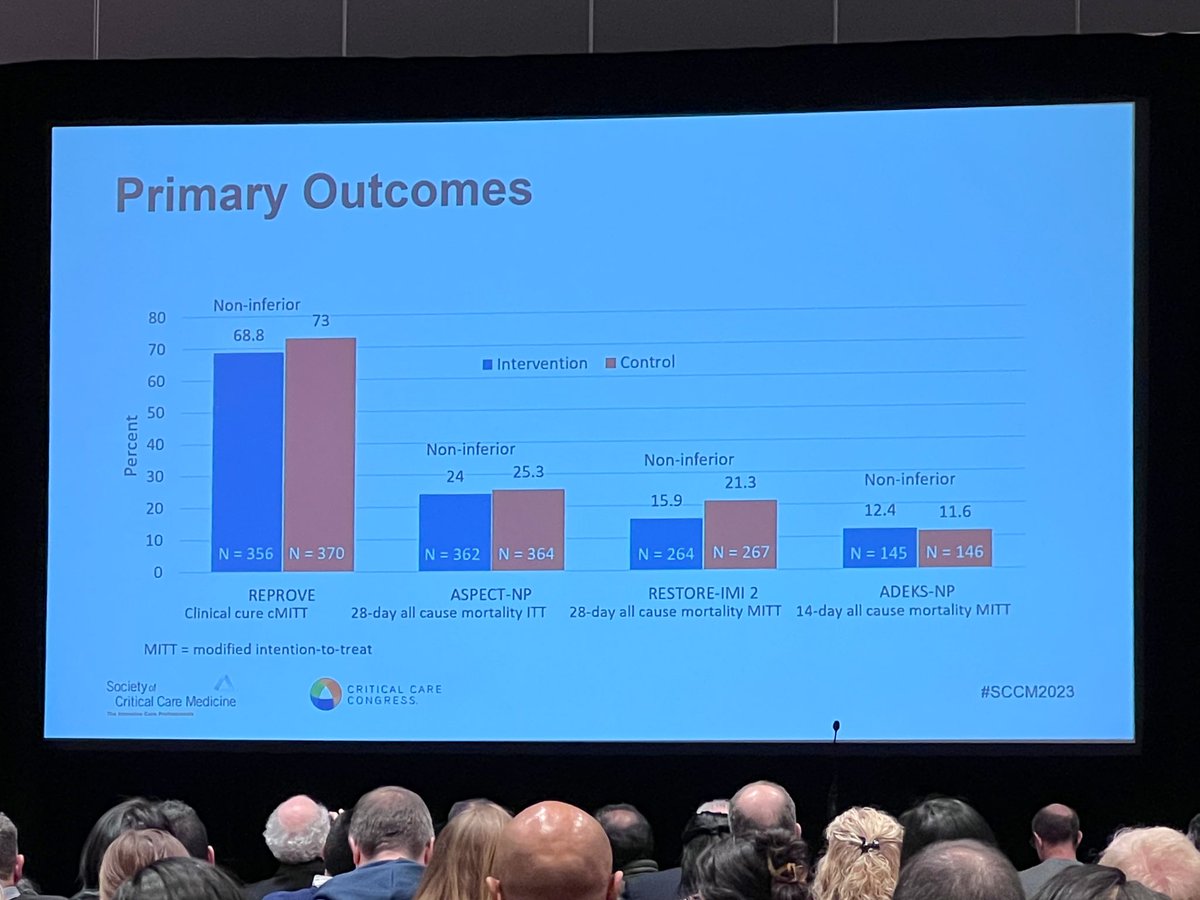
Multiple studies have been published with new antibiotics since the most recent HAP/VAP guidelines were published. These antibiotics were shown as non-inferior in their clinical trials which may result in many alternative options listed in the next guideline update #SCCM2023

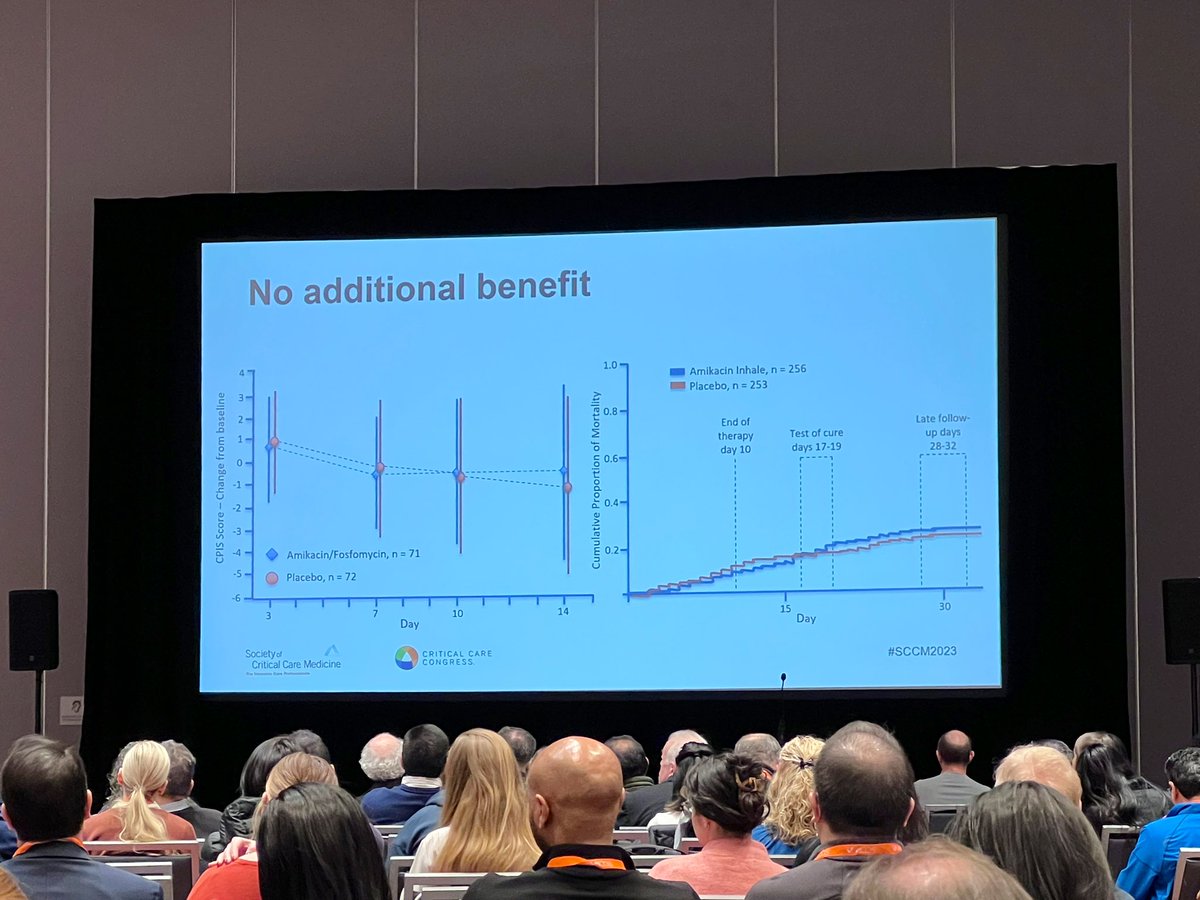
No additional benefit was observed by adding inhaled aminoglycosides in HAP/VAP infections.
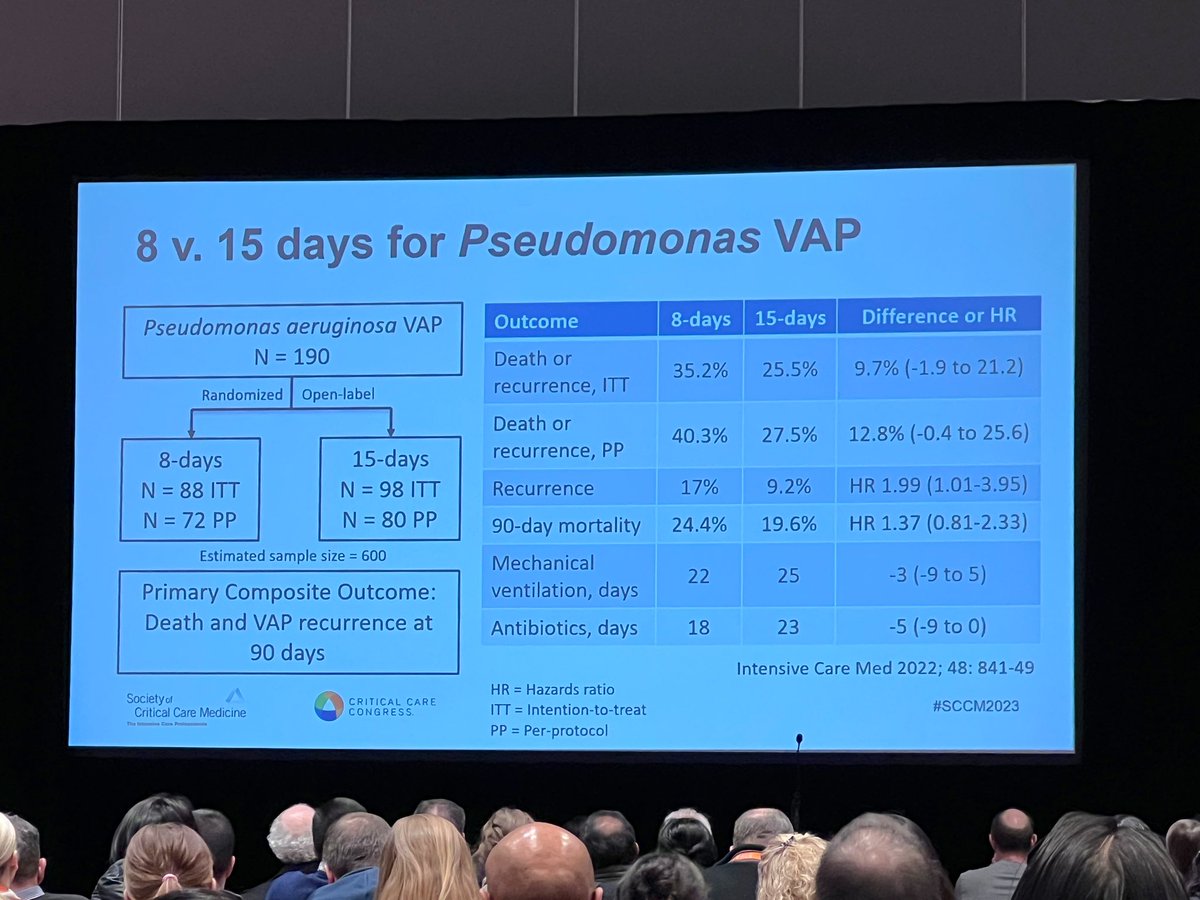
Updates to the Chastre study from the early 2000s failed to show non-inferiority due to recruitment in 8 vs 15 days of treatment for non-fermenter bacterial HAP/VAP infections #SCCM2023
Updates to the Chastre study from the early 2000s failed to show non-inferiority due to recruitment in 8 vs 15 days of treatment for non-fermenter bacterial HAP/VAP infections #SCCM2023
• • •
Missing some Tweet in this thread? You can try to
force a refresh