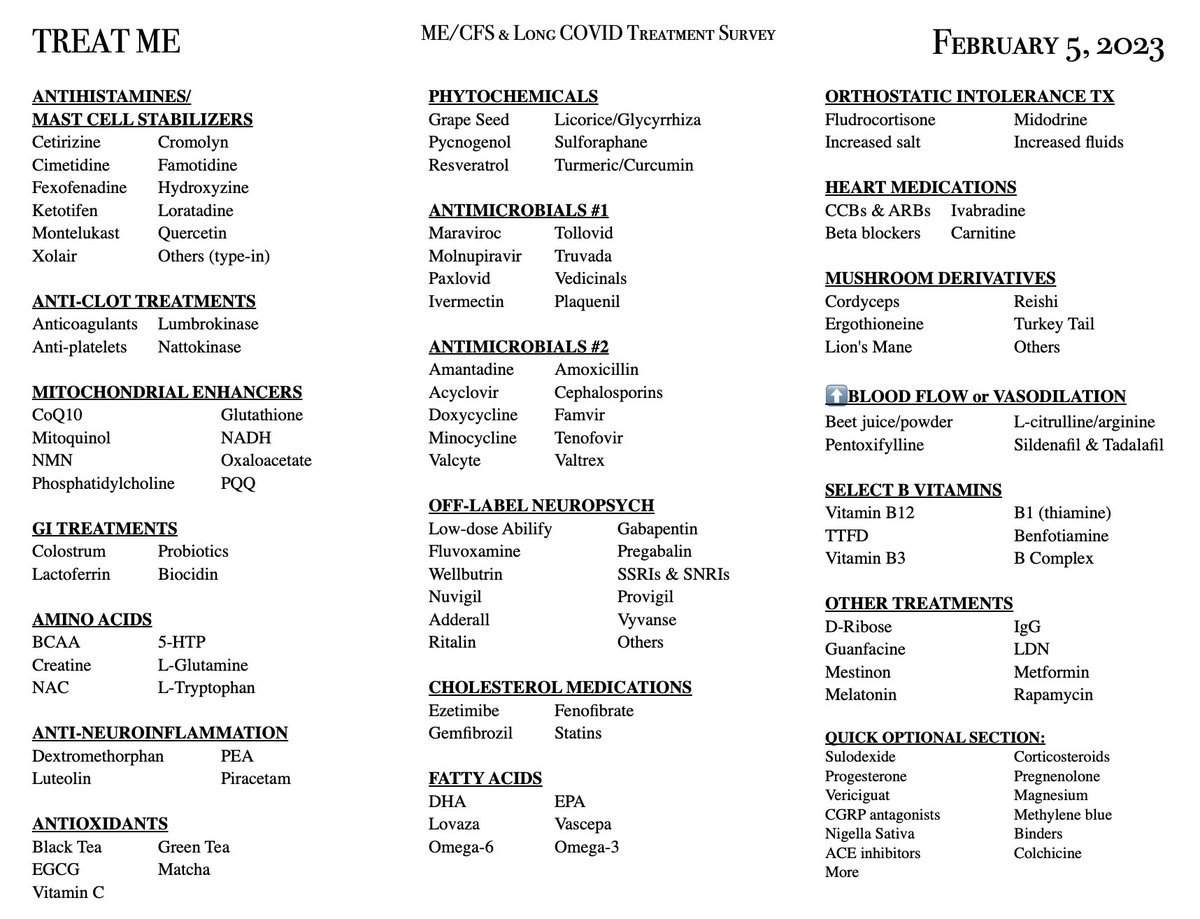
Reviewing preliminary data from the survey (n=1,750!), here are some early observations on a few treatments:
1) Both #pwLC and #pwME benefit remarkably similarly from LDN. Check out the almost identical survey results for overall benefit & number of symptoms improved.
1) Both #pwLC and #pwME benefit remarkably similarly from LDN. Check out the almost identical survey results for overall benefit & number of symptoms improved.




2) People are more likely to benefit from CoQ10 at doses 200 mg or higher, but even then, their overall condition improves only slightly.
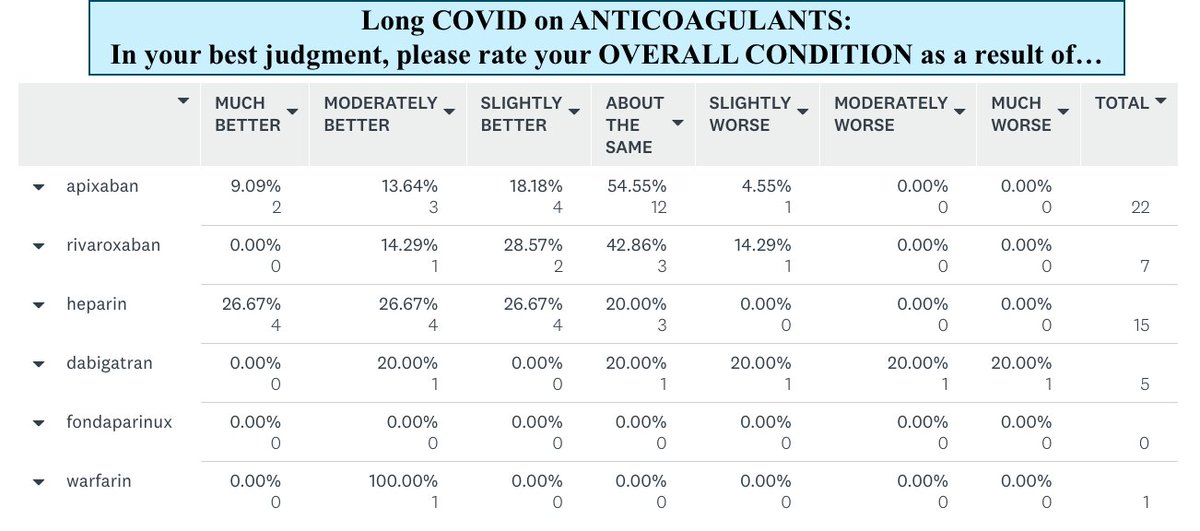
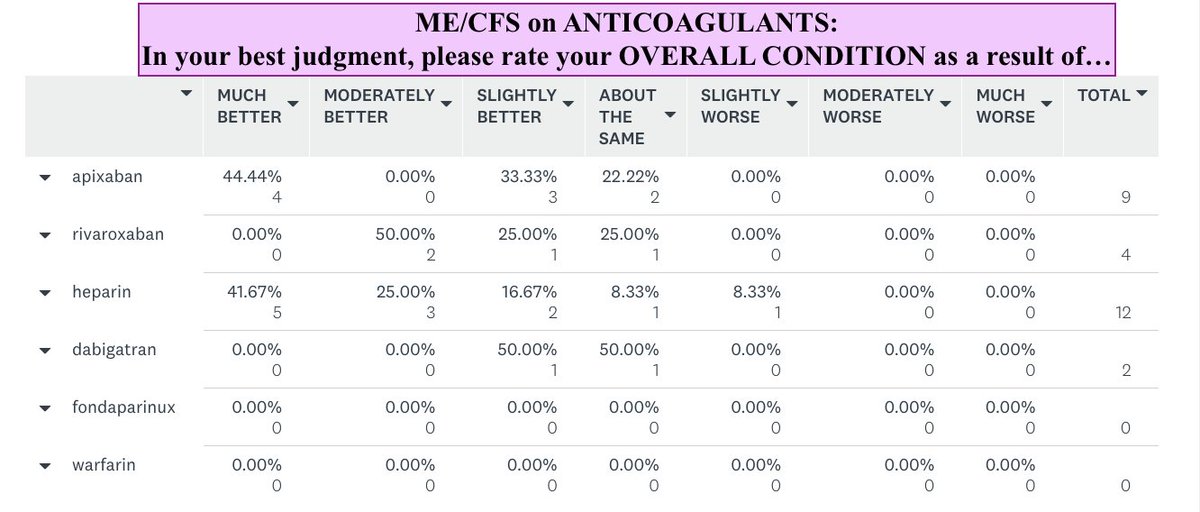
2) Both #pwME & #pwLC benefit from anticoagulants (more on this another time - very interesting stuff!).
2) Both #pwME & #pwLC benefit from anticoagulants (more on this another time - very interesting stuff!).
3) There is a clear increase in benefit when adding on antiplatelets to anticoagulants, but aspirin alone does not help many (78/255).
4) Interestingly, HEPARIN may be more beneficial in both pwME & pwLC than direct oral anticoagulants.
4) Interestingly, HEPARIN may be more beneficial in both pwME & pwLC than direct oral anticoagulants.

5) The majority of ME/CFS respondents have had ME for over 20 years. 😢
6) The majority of LC respondents have had LC for 6-12 months.
7) NAC dose: Only 29% of those on NAC ≤600 mg daily had sustained benefits (n=195) compared to 51% on NAC >600 mg daily (n=106)
6) The majority of LC respondents have had LC for 6-12 months.
7) NAC dose: Only 29% of those on NAC ≤600 mg daily had sustained benefits (n=195) compared to 51% on NAC >600 mg daily (n=106)
8) Those on primarily EPA supplements reported more benefits than those on mixed fatty acid (DHA+EPA).
9) The majority (~60%) of those who started NK, LK and/or SP did not report any Herxheimer effects or worsening of symptoms at beginning of treatment.
9) The majority (~60%) of those who started NK, LK and/or SP did not report any Herxheimer effects or worsening of symptoms at beginning of treatment.
10) The most commonly-used proteolytic enzyme brand = Doctor's Best NK (n=106), with Natto-Serra the 2nd-most used (n=94).
11) 15% (23 in 134), 10% (5/48) and 7.7% (8/104) of those with MCAS reported worsening of MCAS symptoms with NK, LK, & SP, respectively.
11) 15% (23 in 134), 10% (5/48) and 7.7% (8/104) of those with MCAS reported worsening of MCAS symptoms with NK, LK, & SP, respectively.
12) Proteolytic enzymes (NK, LK, SP) was an uplifting treatment section to review. I need to spend a lot more time analyzing the results but here's some raw data. Nice to see that 11.6-13.6% reported feeling MUCH better on NK, LK, or NK/SP combo.

13) While most people reported benefits from melatonin (n=343), unfortunately the majority reported that only ONE symptom improved (related to sleep).
14) Of the 27 who trialed GUANFACINE, around half reported benefits, with brain fog & sleep improving the most. See raw data.
14) Of the 27 who trialed GUANFACINE, around half reported benefits, with brain fog & sleep improving the most. See raw data.


15) Sadly, very few #pwLC seem to be able to access antivirals. The sample sizes are on the low side but in general the vast majority (~70-80%) who improved on them report that they lost at least some or even all benefits after stopping therapy.
For those who wanted to take the survey a 2nd time for a loved one and/or child but had trouble, here is a link to a fresh link / COPY of the survey. For the 20 #pwME who were kicked out of the survey due to a glitch 2 days ago, please use this link!
surveymonkey.com/r/COPYOFTREATME
surveymonkey.com/r/COPYOFTREATME
• • •
Missing some Tweet in this thread? You can try to
force a refresh