
1/Can you ACE this #MedEd & #TwitteRx #Tweetorial on non-allergic drug-induced angioedema? 57yof w/ swelling of face, lips, and tongue w/ no urticarial rash. Meds: valsartan, sacubitril, metformin, simvastatin, sitagliptin, & risperidone. How many meds may be contributing? 

2/Drug-induced angioedema (DIA) can be divided into 2 categories
1⃣ Allergic DIA: IgE-mediated release of histamine from mast cells
2⃣ Non-allergic DIA: Increased vascular permeability mostly from disruption of the kallikrein-kinin system (KKS)
1⃣ Allergic DIA: IgE-mediated release of histamine from mast cells
2⃣ Non-allergic DIA: Increased vascular permeability mostly from disruption of the kallikrein-kinin system (KKS)

3/For non-allergic mediated DIA, easiest to think about changes in bradykinin (BK) activity
🥇- 👇metabolism of BK (and substance P)
🥈- 👆BK production
🥉- 👆BK receptor activity
🥇- 👇metabolism of BK (and substance P)
🥈- 👆BK production
🥉- 👆BK receptor activity
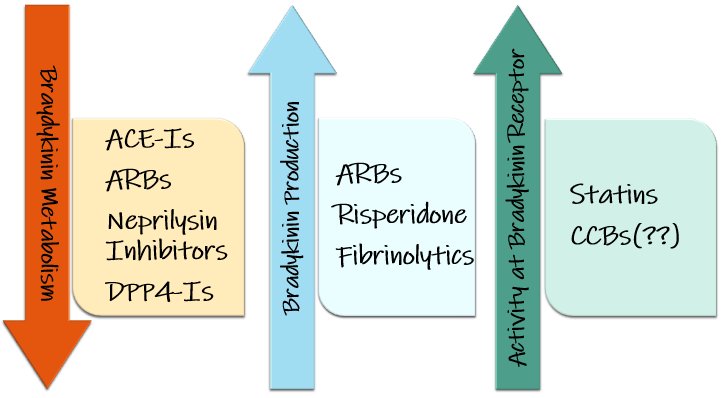
4/🥇It's more than just ACE! ACE and Neprilysin both metabolize BK, & DPP4 breaks down inactive BK. PLUS all 3 enzymes also metabolize substance P which 📈 vascular permeability. ACE and Neprilysin inhibitors have greatest risk, but DPP4-Is may "tip the⚖️" if on ARNI or ACE

5/🥇&🥈Incidence with ARBs < ACE, but can still cause DIA. Blockade of A2R signals for upregulation of AngII potentially causing 📈kallikrein activity to initiate RAAS &📉 ACE activity to limit AngII metabolism

6/🥈tPA can also cause DIA, as plasmin activation leads to 📈XIIa which 📈kallikrein which 📈BK! Though rare, risperidone (PMC5906767) may 📉c1-esterase inhibitor which acts as the brakes for KKS by🛑kallikrein and🛑XIIa.

7/🥉Again rare (PMC6135297), but statins can📈expression of BK2 receptors which when combined with meds from 🥇may cause DIA. Lastly the MOA for CCBs is not well described but may be due to📈NO production that potentiates the effects of BK2 stimulation

8/So did you ACE the case? Everything but metformin may be contributing to DIA in this patient. Next time someone says “it's ACE-induced angioedema”, make sure to look for other potential drugs that may be tipping the ⚖️!

@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh



