Y'all ready for this? 🍿👊
#NarcanAdCom about to pop off
Use this # to follow today's updates
CONCEPT
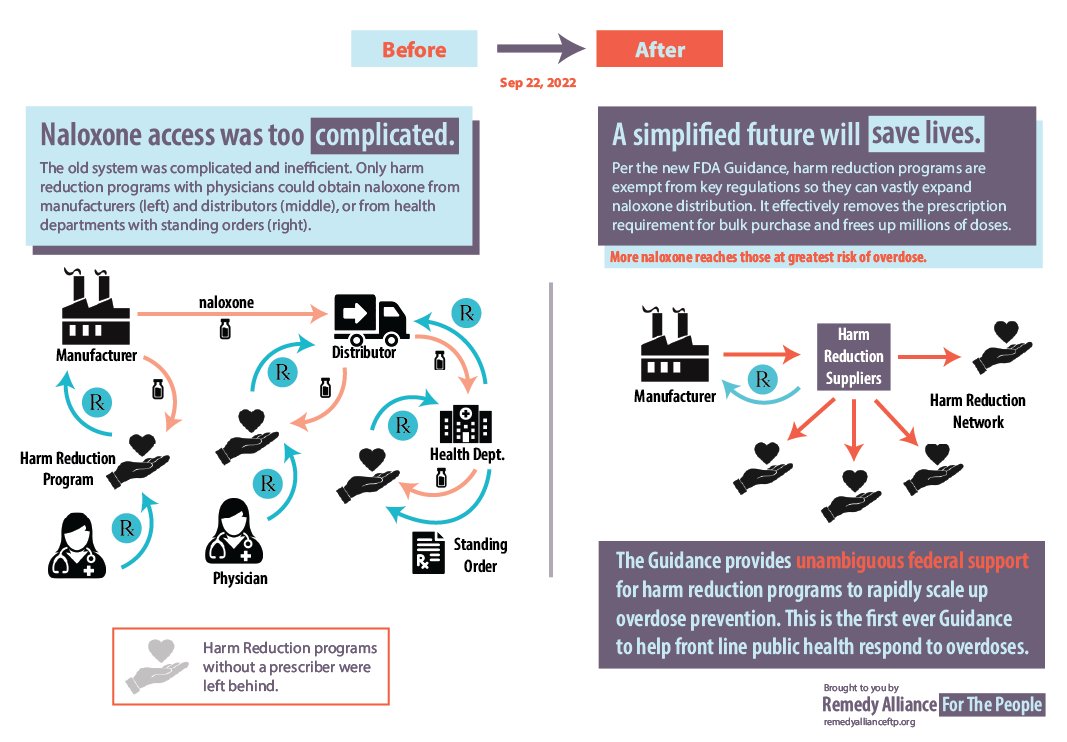
The culmination of 2 decades of advocacy to make naloxone OTC
REALITY
2 decades of advocacy erased by overdose crisis profiteers $EBS
#NarcanAdCom about to pop off
Use this # to follow today's updates
CONCEPT
The culmination of 2 decades of advocacy to make naloxone OTC
REALITY
2 decades of advocacy erased by overdose crisis profiteers $EBS
Right out the gate, FDA frames this as a solution for saving kids from overdose. Guess that’s why there are so many pediatric anesthesiologists on the AdCom
In the review of the history FDA forgets to credit the people (like Dan Bigg) who invented the intervention
The “misbranded” — translation: State Boards of Pharmacy won’t let pharmacies sell naloxone OTC until the Rx labeled boxes are out of the supply chain 

Calling out the first lie — IM naloxone has decades of experience for layperson use SUCCESSFULLY. Again erasure is the theme of the day.
Let's be clear -- @US_FDA stole the intellectual property of @ChiRecoveryAlli to create the OTC instructions, used it without attribution, and then handed it to $EBS to make billions off of. Erasure of civil society is shameful, but par for the course.
#NarcanAdCom
#NarcanAdCom

In their opening statement $EBS reminds us of their manufacturing prowess
nytimes.com/2022/05/10/us/…
nytimes.com/2022/05/10/us/…
$EBS: "Narcan doesn't need training" -
But neither does IM naloxone, as decades of experience have shown.
But neither does IM naloxone, as decades of experience have shown.
Calling $EBS out on their lies - Community based distribution started in 1996, not 2008.
ERASURE
ERASURE
ERASURE
#NarcanAdCom
ERASURE
ERASURE
ERASURE
#NarcanAdCom

"EmBi wanted to make it available to be people most at risk of OD."
Right. That's why you donated how many doses exactly?
Right. That's why you donated how many doses exactly?
$EBS strategy is classic pharma -- expand to new populations to make more money. OD deaths among young adults is a tragedy. They are, mercifully, a relatively small portion of overdose deaths.


$EBS leaning heavy into typical Drug War "Save the Kids" trope. Classic.
Here are the advisors at the #NarcanAdCom who will decide on OTC naloxone.
Plenty of pediatric anesthesiologists but ZERO community based harm reduction expertise.
fda.gov/media/165413/d…
Plenty of pediatric anesthesiologists but ZERO community based harm reduction expertise.
fda.gov/media/165413/d…
$EBS making it clear they want to market to the affluent. Rich folks 2-out-3 people in their study had $50,000+ household income.

Did Vyas just say 44 million doses of Narcan have been distributed? Where did this number come from??
Proposed new instructions from on the larger carton box that $EBS wants to use. The current box is already so large that a friend had to buy a larger purse to carry it around.

Dr Higgins: Was anything new learned from human factors study?
$EBS: People liked being able to see back panel first, so get it all on one page
$EBS: People liked being able to see back panel first, so get it all on one page
There is conflict between traditional and $EBS versions of instructions -- @cdc says to call 911 FIRST, but $EBS puts it second. So, will health departments have to redo their training material?

@DrScottHadland "Education is still important with OTC"
"2 doses is enough"
"2 doses is enough"
That your wife is a lawyer isn’t a qualification to ask about long-settled legal liability questions. She got teh degree, not you. Do your homework, this has been well-addressed already.
bjatta.bja.ojp.gov/tools/naloxone…
bjatta.bja.ojp.gov/tools/naloxone…
Question from Parker now about how much expiration date matters. Are these "experts" really so inexperienced? These are routine questions that have been addressed years ago.
“Is expiration date on outside of carton?”
Seriously it’s like these Advisors have never held a box of Narcan in their hands
Seriously it’s like these Advisors have never held a box of Narcan in their hands

New proposed box 45% larger

Dr. Jacobson from Ri provides definitive answer that one dose is enough, but that OTC could allow more boxes per patient! 🤔
Naloxone sales data from IQVIA via FDA. They repeatedly caveat that these data do not include harm reduction data.


$EBS phramacovigilance data. Millions of doses sold, and only <400 safety reports



Product use errors with Narcan Rx — keep an eye on this as it goes OTC. Flonase experience is really applicable here, where medication errors went waaaaay up after OTC switch.

And now Cohen brags about @DrWoodcockFDA stealing the naloxone OTC label from the community and publishing it in NEJM. @RemedyAlliance
Dan, I'm sorry.
Dan, I'm sorry your brilliant work was stolen.
Dan, I'm sorry you're not hear to tell them what's up.
Dan, I'm sorry.
Dan, I'm sorry your brilliant work was stolen.
Dan, I'm sorry you're not hear to tell them what's up.

$EBS originally tried to make the OTC version (right) cheaper by taking away the quickstart instructions, but now they propose to add back. This kind of paper-in-blister is more expensive, costs passed along to OTC patients. "Safe use" has a price tag.

Despite the opening salvo of SAVE THE KIDS, the real scientists at FDA point out that the instructions weren't reliably tested by $EBS on teenagers. We see clear disconnecting btwn marketing rhetoric vs. company's science. FDA just called them out.

THIS is why IM naloxone won't be OTC.
Standard here for OTC is incredible high bar. FDA going thru every little stumble with the instructions.
Look, there will never be 100% perfection, especially in actual OD situations. ... this nitpicking is responsible regulation, but also… twitter.com/i/web/status/1…
Standard here for OTC is incredible high bar. FDA going thru every little stumble with the instructions.
Look, there will never be 100% perfection, especially in actual OD situations. ... this nitpicking is responsible regulation, but also… twitter.com/i/web/status/1…
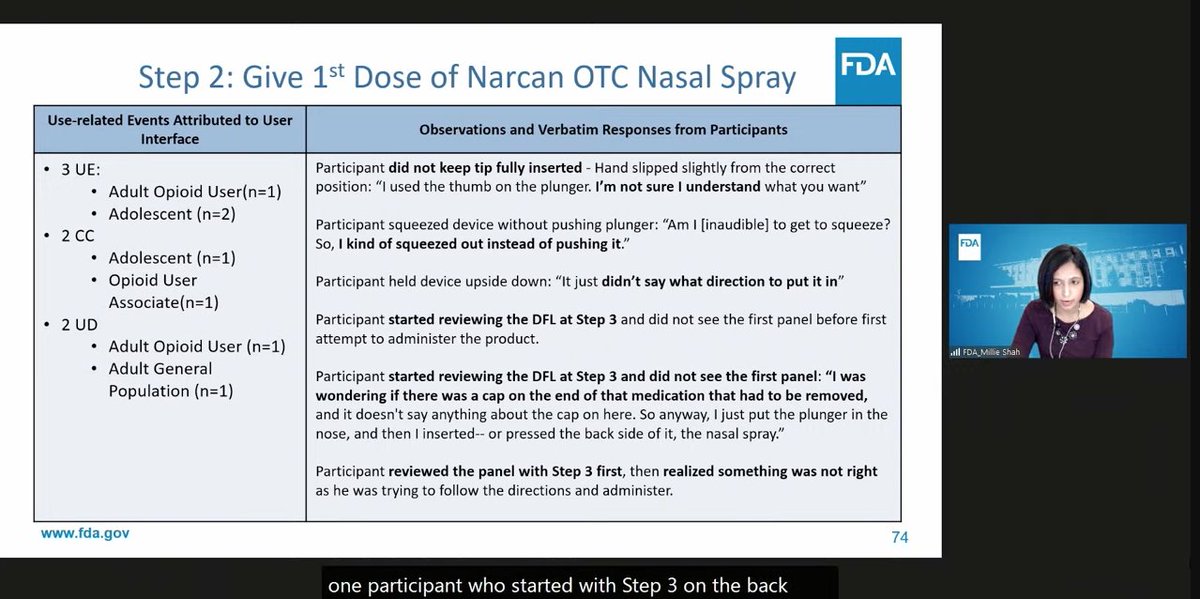

A few dozen participants in a contrived instruction-understanding study
trump
decades of actual community use success
trump
decades of actual community use success
And now, the Advisors will group-wordsmith & micro-edit the instructions. Have you even tried to edit a doc as a group? Thank god so many of the Advisors have extensive design experience! "Can we get a Word version?"
Advisor: "But you didn't study kids. What about kids who can't read? Shouldn't they be able to see the pictures and administer naloxone?"
Wait, FDA just opened the door to $EBS having to redo the study on the instructions?? YIKES.
Clement: "FDA have you ever thought about if two people are there to reverse OD. What happens when there is 2 people in the room?"
FDA: Impossible to measure.
Harm Reductionists: Yeah, it works fine. Fix Good Sam laws now, please.
FDA: Impossible to measure.
Harm Reductionists: Yeah, it works fine. Fix Good Sam laws now, please.
Public comments kick off with an anesthesiologist who uses fentanyl in clinic, but also lost 2 sons to overdose, and administered naloxone. Strongly supports OTC. Points out how awful police can be who said of her son "don't know why we waste ReviveMe.com… twitter.com/i/web/status/1…
Anesthesiologist repeats that single dose is enough.
Dr. Bonnie Milas: "Current free access to naloxone must be increased. Mail-to home is simplest, least stigma." Calls for corporate cooperation.
@BonnieMilas: "My sons are never coming home. Life is precious and slips away quickly. OTC naloxone is the next game changer. The time is now."
@BonnieMilas Great comments from Addiction Policy Forum:
"Should be as easy as Tylenol."
Warns of 3 unintended consequences:
1. Change to OTC doesn't access for free to high risk pops. OTC supplement not supplant current harm reduction distribution. Keep ACTIVE distribution, vs. PASSIVE… twitter.com/i/web/status/1…
"Should be as easy as Tylenol."
Warns of 3 unintended consequences:
1. Change to OTC doesn't access for free to high risk pops. OTC supplement not supplant current harm reduction distribution. Keep ACTIVE distribution, vs. PASSIVE… twitter.com/i/web/status/1…
Next @fwbrason2 @ProLazNC -- first pharmacy naloxone distribution happened in Wilkes County NC at Brame Huie Pharmacy by Kathy Huie. We started this in 2008. And just now looking at OTC, 15 years later. What's the best way to get naloxone out to general public? Look at current… twitter.com/i/web/status/1…
@fwbrason2 @ProLazNC Speaker 6 - Spangler @CHPA
Only a few OTC products can save lives (aspirin, nicotine replacement, etc.). Re: naloxone... Now is the time to finish the job. OTC will help counter stigma of interacting with healthcare professional, and help harm reduction purchasing in bulk.
Only a few OTC products can save lives (aspirin, nicotine replacement, etc.). Re: naloxone... Now is the time to finish the job. OTC will help counter stigma of interacting with healthcare professional, and help harm reduction purchasing in bulk.
That's it. Only 6 public comments. No representation from on the ground harm reduction programs -- their silence and absence speaks volumes. This is OTC switch is clearly intended for general population, not harm reduction.
Back to the Advisors. Pisarik: "What else could folks be doing if not an OD, like diabetic coma or heart attack? Not trying to train public on being 1st responders. Wording in label SHOULD YOU BE DOING RESCUE BREATHING OR CPR?"
This is a big departure in the instructions -- no… twitter.com/i/web/status/1…
This is a big departure in the instructions -- no… twitter.com/i/web/status/1…
Coyle: "This is administered to patient who may not know about naloxone. What are other issues?"
Michele: "Need to make instructions as simple as possible."
Michele: "Need to make instructions as simple as possible."
Clement: "How much education is really needed? How much should be put in label? Are there other ways $EBS can educate lay public? Can they put videos on their website?"
As if harm reduction programs haven't been doing this for decades already. Again, ERASURE is the theme of the… twitter.com/i/web/status/1…
As if harm reduction programs haven't been doing this for decades already. Again, ERASURE is the theme of the… twitter.com/i/web/status/1…
Michele: "We boiled this all down to "Call 911." Consumers will need lots of education and info.
We rely on the community at large. They are incredible valuable resources, academics and clinicians."
Again, erasure of harm reduction programs who have been the front line for… twitter.com/i/web/status/1…
We rely on the community at large. They are incredible valuable resources, academics and clinicians."
Again, erasure of harm reduction programs who have been the front line for… twitter.com/i/web/status/1…
Ness: "Moral obligation of companies selling this medication to provide connection to care. Can there be a website connection?"
Michele: No REMS for OTC drugs
Let's review -- Connection to care was REQUIRED for harm reduction programs by worried policymakers. But FDA giving… twitter.com/i/web/status/1…
Michele: No REMS for OTC drugs
Let's review -- Connection to care was REQUIRED for harm reduction programs by worried policymakers. But FDA giving… twitter.com/i/web/status/1…
Green from FDA gives charge to committee.
Here are the questions to be asked:
Notice the lack of any consideration of the impact on harm reduction programs who form the backbone of naloxone distribution in the US.
Here are the questions to be asked:
Notice the lack of any consideration of the impact on harm reduction programs who form the backbone of naloxone distribution in the US.

☎️ Hello double standards!! Striking that 2 key things that harm reduction programs have been forced to do are not being asked of pharma.
1. Call 911 before giving naloxone
2. Connecting people to drug treatment
1. Call 911 before giving naloxone
2. Connecting people to drug treatment
• • •
Missing some Tweet in this thread? You can try to
force a refresh