
Tweetorial on sub-typing non-small cell lung carcinoma in cytology samples - essentially, how to tell a squamous carcinoma from an adenocarcinoma.
The most important distinction at the moment is "Could this be (in whole or in part) an adenocarcinoma?", given the additional ancillary tests typically done on adenocarcinoma and typically not done on squamous carcinoma.
There are many descriptions of the *features* of either entities, but what are the *criteria* that can be used to definitively type as adenocarcinoma or squamous carcinoma?
For adenocarcinoma:
- Acinar formations; the nuclei are in the periphery, the border is often (though not always) smooth, the cytoplasm toward a central point
- Acinar formations; the nuclei are in the periphery, the border is often (though not always) smooth, the cytoplasm toward a central point

- Mucin vacuoles; with peripheral reinforcement, very round shape, sometimes indenting the nucleus; most convincing when there's "targetoid" mucin in the centre of the vacuole



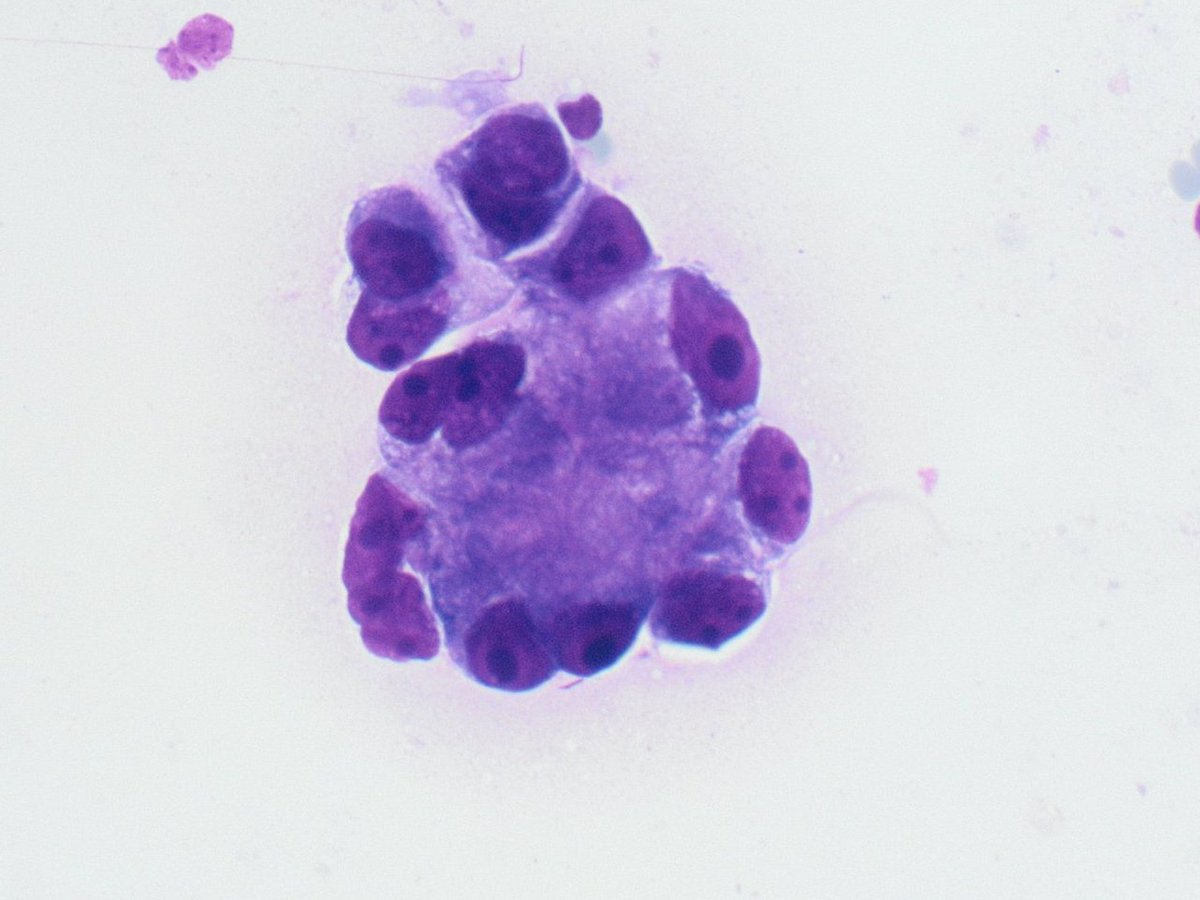
- Flat sheets, particularly in a case like this one, where more overtly malignant features can be seen elsewhere. These will typically be only in pulmonary specimens, because they represent a lepidic component

Of course, these flat sheets have to be malignant, so look for the absence of cilia, and for either all mucinous cells or no mucinous cells - alternating mucinous and non-mucinous suggests normal epithelium.
And I would add intact papillary structures, if ever I actually saw one in an FNA specimen.
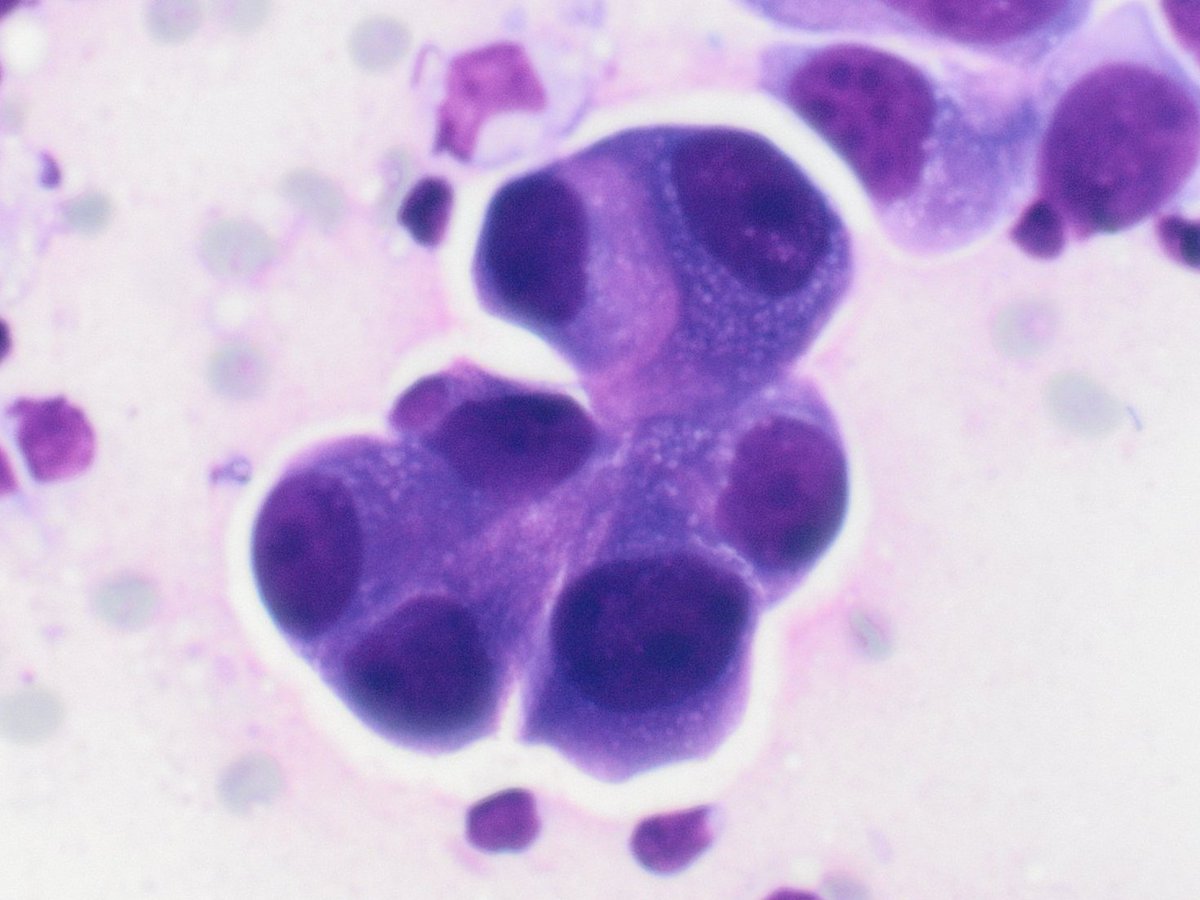
What are NOT criteria, even though they're generally features of adenocarcinoma:
- Prominent nucleoli
- Relatively monomorphic (but enlarged) nuclei
- Vaguely eccentric cytoplasm
Here's a nice case of squamous carcinoma:
- Prominent nucleoli
- Relatively monomorphic (but enlarged) nuclei
- Vaguely eccentric cytoplasm
Here's a nice case of squamous carcinoma:


As for the criteria to find squamous differentiation:
- Keratin pearls (notice the photomicrograph from my Twitter banner)
- Keratin pearls (notice the photomicrograph from my Twitter banner)



- Orangeophilia

And in Romanowsky stains (because it isn't true you can't see squamous differentiation with these), Robin's egg blue


What are NOT criteria, even though they're generally features of squamous carcinoma:
- Marked variation in nuclear size among the malignant cells
- Streaming nuclei
- Necrosis
- Marked variation in nuclear size among the malignant cells
- Streaming nuclei
- Necrosis
Note that here, I'm only calling "criteria" the same types of things that are used in surgical pathology. Surgical pathologists don't look at prominent nucleoli, and type as adenocarcinoma - and neither should we in cytopathology.
If none of these criteria can be found, just do the stains (but not a million of them!).
As always, hope you'll find this useful. Please RT if you have. Let me know if you think I missed anything.
• • •
Missing some Tweet in this thread? You can try to
force a refresh








