
Please don't put out poorly thought out 'research' like this- These comparisons are heavily flawed and serve only to massively underestimate the impact of long COVID & serve abelist narratives. 🧵 
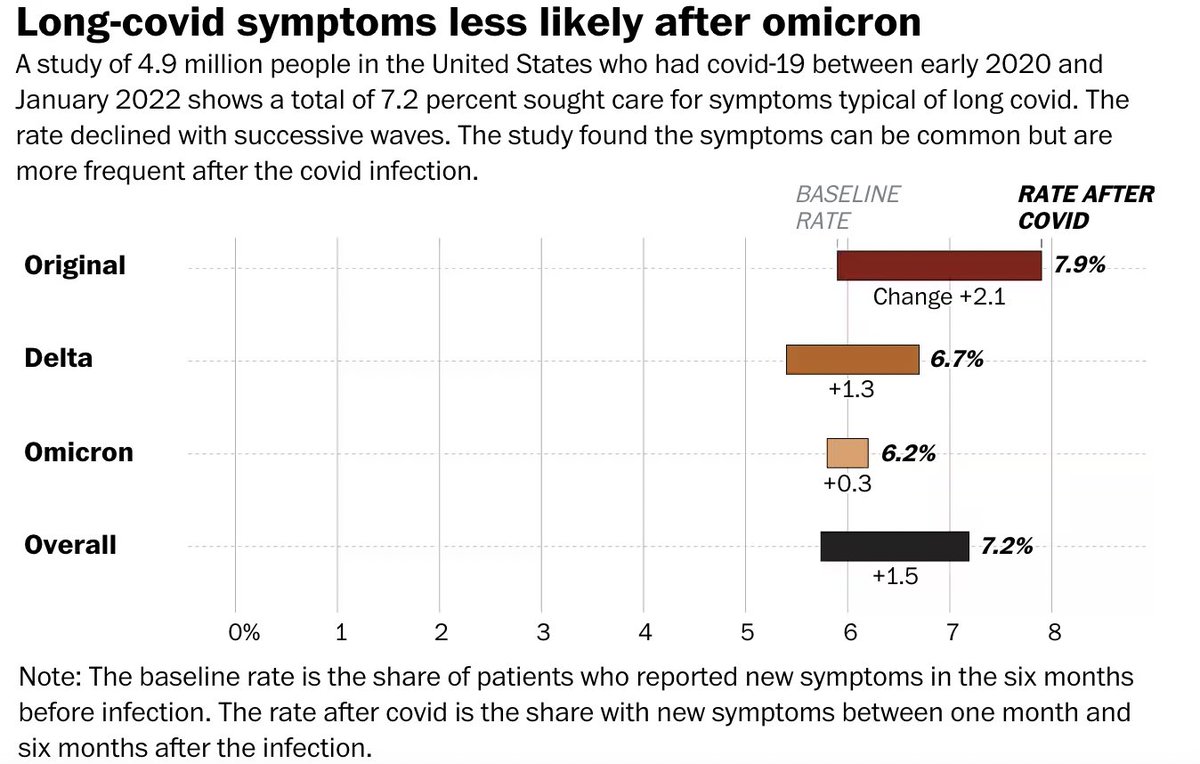
first of all - baseline rate? I've discussed before why using this 'control' rate is deeply problematic and will always underestimate the true prevalence of long COVID. I've written about this many times:
https://twitter.com/dgurdasani1/status/1487578265187405828?s=20
In fact these comparisons lead to a familiar paradox that I've highlighted before where the difference in prevalence for a single symptom (e.g. loss of smell) is lower that the calculated prevalence of long COVID based on the 'any symptom' definition for all symptoms.


This should not be possible - the incidence of a single symptom of long COVID *should not* be lower than the incidence of long COVID overall. I've illustrated this before with ONS data
https://twitter.com/dgurdasani1/status/1498393645686394886?s=20
Why does this paradox happen? Because
-syndromes are constellations of symptoms, not a single one
-many people who have pre-existing conditions get long COVID - but would not be counted in the difference in prevalence comparison because they had one of the symptoms at baseline
-syndromes are constellations of symptoms, not a single one
-many people who have pre-existing conditions get long COVID - but would not be counted in the difference in prevalence comparison because they had one of the symptoms at baseline

So, if you have 40% of people who have any one of the symptoms you're measuring, then by definition, if you define prevalence as 'prevalence of any symptom in cases minus prevalence of any symptoms in controls', this group can't develop long COVID (filled circles in image).

But in reality, this is the group that has the highest risk of developing long COVID - but these prevalence estimates don't count them at all. So if the people with baseline symptoms (filled blue circles above) developed long COVID, they simply wouldn't count in these estimates.
Second, infection rate following omicron has been higher than with any other variant- what about absolute numbers? So even if the probability of getting long COVID post omicron was - say - halved, if probability of infection was doubled, the absolute numbers would still be same
Basic math. In truth, infection rates post omicron haven't just doubled- in many parts of the world because mitigations have been dropped, and omicron subvariants are highly transmissible and have high immune escape, infection rates have increased several fold.
So the incidence of long COVID post-COVID would have to decline substantially in the omicron wave for this not to have an impact.
So tired of reading poorly thought out narratives that pretend to be evidence when there is absolutely no thought to understanding the syndrome, and how to design a study that actually does this.
Also, how is long COVID incidence assessed- it's not just about people seeking care for this. Long COVID disproportionately affects groups that are disabled, with pre-existing conditions, and disadvantaged. We know that a lot of people with long COVID don't seek care.
Often care isn't even accessible. Systematic surveillance of a broad range of symptoms is needed- with clear comparisons to baseline rather than just looking at people accessing care.
In fact if you know anything about long COVID risk factors, you also know that those who are at greatest risk are least likely to be able to access care. Such studies aren't just bad science, they're also abelist
because they ignore that those who have pre-existing conditions also get long COVID, and ignore the massive barriers to care for long COVID- especially among the disabled, chronically ill, and socio-economically disadvantaged who are most likely to get it in the first place.
Also notable that there's no assessment of post-COVID sequlae here- higher risk of diabetes, cardiovascular disease, clotting, renal disease, pulmonary embolism and so many other chronic illnesses known to be associated with COVID long term.
No surprise though that this will be used in bad faith as it has by those who have consistently undermined the case for mitigations and protections
https://twitter.com/docalisaNY/status/1637425550842118145?s=20
If I developed long COVID - in these comparisons, I wouldn't count- because I had symptoms like fatigue at baseline. It doesn't matter that I have had significant worsening of this, and POTS to the point that it's limiting my day to day activities - it still wouldn't count.
Because I'd be buried in the 'baseline' as per these estimates. There are so many others like me - who had one of the many symptoms measured at baseline, but their health has significantly worsened post-COVID. They've developed new symptoms or worsening of previous ones.
Yet, a difference is prevalence from 'baseline' - a method so commonly used and published by 'experts'- wouldn't include them.
But they should count. The big question is really why we design research in a way that does this?
But they should count. The big question is really why we design research in a way that does this?
• • •
Missing some Tweet in this thread? You can try to
force a refresh




