
💎 of #ApexPathshala
Dr. Patrick Walker takes a deep dive into the history of ‘MPGN’ as a nebulous entity eluding understanding for decades.
Here’s his meandering tale of MPGN that begins in early 1900s & goes on till the turn of the century.🧵
#historyofmedicine #nephtwitter
Dr. Patrick Walker takes a deep dive into the history of ‘MPGN’ as a nebulous entity eluding understanding for decades.
Here’s his meandering tale of MPGN that begins in early 1900s & goes on till the turn of the century.🧵
#historyofmedicine #nephtwitter
1914
Dr.Theodor Fahr,the first modern pathologist & Dr.Franz Volhard,an internist from Mannheim🇩🇪,undo many prevailing misconceptions through formative work on Bright’s disease.
Their book👇🏻‘Die Bright’sche Nierenkrankenheit’ becomes a classic in the annals of glomerulology.2/n
Dr.Theodor Fahr,the first modern pathologist & Dr.Franz Volhard,an internist from Mannheim🇩🇪,undo many prevailing misconceptions through formative work on Bright’s disease.
Their book👇🏻‘Die Bright’sche Nierenkrankenheit’ becomes a classic in the annals of glomerulology.2/n

1960s
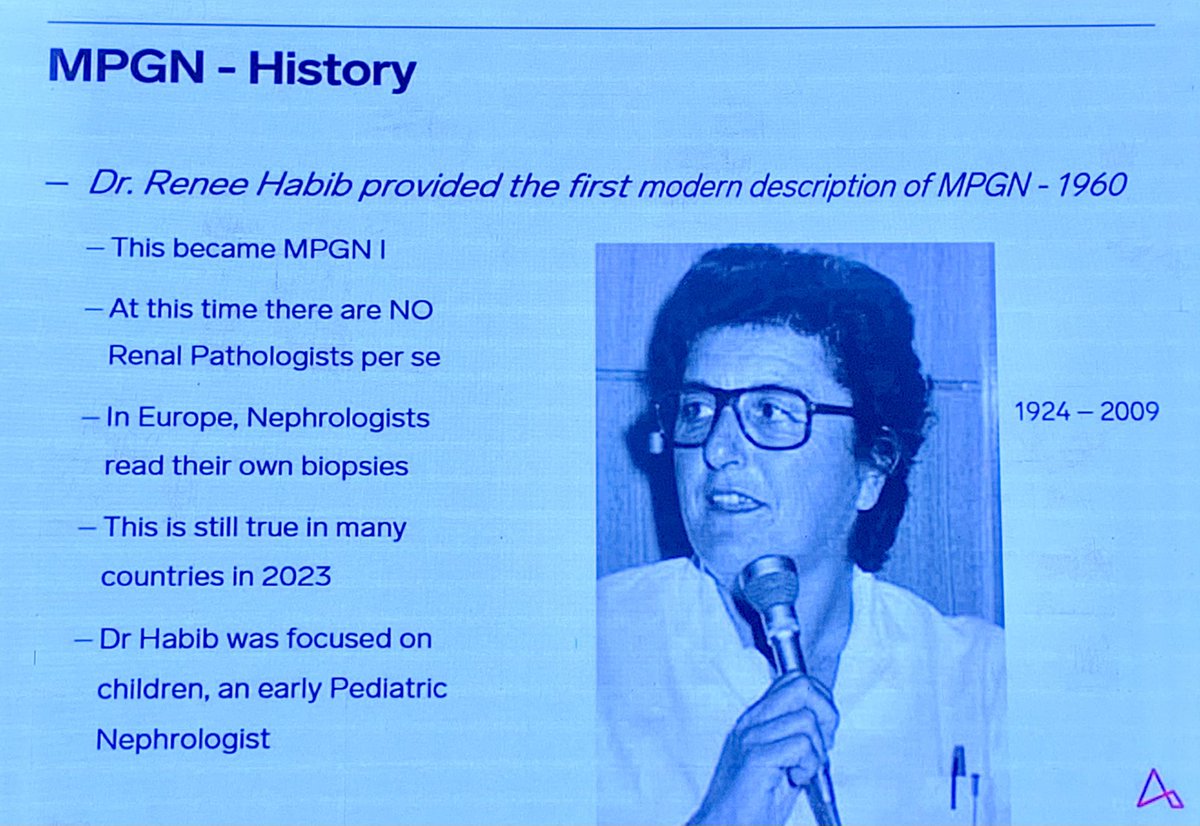
Dr. Rene Habib,a pioneering pediatric nephrologist,studies a large cohort of children with MPGN &provides first descriptions of the disease.
Clinical & histopathological features of what formally gets named as MPGN l at the CIBA symposium convened at London in 1961. 3/n
Dr. Rene Habib,a pioneering pediatric nephrologist,studies a large cohort of children with MPGN &provides first descriptions of the disease.
Clinical & histopathological features of what formally gets named as MPGN l at the CIBA symposium convened at London in 1961. 3/n
The CIBA symposium is the first of its kind in the world- a meeting of renal pathologists🔬& renal clinicians🩺 with a cumulative experience of 5000 biopsies, discussing various forms of glomerulonephritides.
Metaphorical🚂 ➡️ progress 4/n
Metaphorical🚂 ➡️ progress 4/n

1970s
Enter the complement 🐉
Dr. Clark West et al, quantify C3, C3 nephritic factor and factor B levels in MPGN at Cincinnati, OH.
ncbi.nlm.nih.gov/pmc/articles/P…
5/n
Enter the complement 🐉
Dr. Clark West et al, quantify C3, C3 nephritic factor and factor B levels in MPGN at Cincinnati, OH.
ncbi.nlm.nih.gov/pmc/articles/P…
5/n

Meanwhile in 1960s
🔍Dense deposit disease (DDD) is first described by Dr. Jean Berger👇🏻& Dr. Galle. They publish the findings in multiple papers to increase the scientific reach.
Dr. Walker’s poetic ‘Charcoal smudge versus calligraphy line’ analogy here.👇🏻6/n
🔍Dense deposit disease (DDD) is first described by Dr. Jean Berger👇🏻& Dr. Galle. They publish the findings in multiple papers to increase the scientific reach.
Dr. Walker’s poetic ‘Charcoal smudge versus calligraphy line’ analogy here.👇🏻6/n


1970s
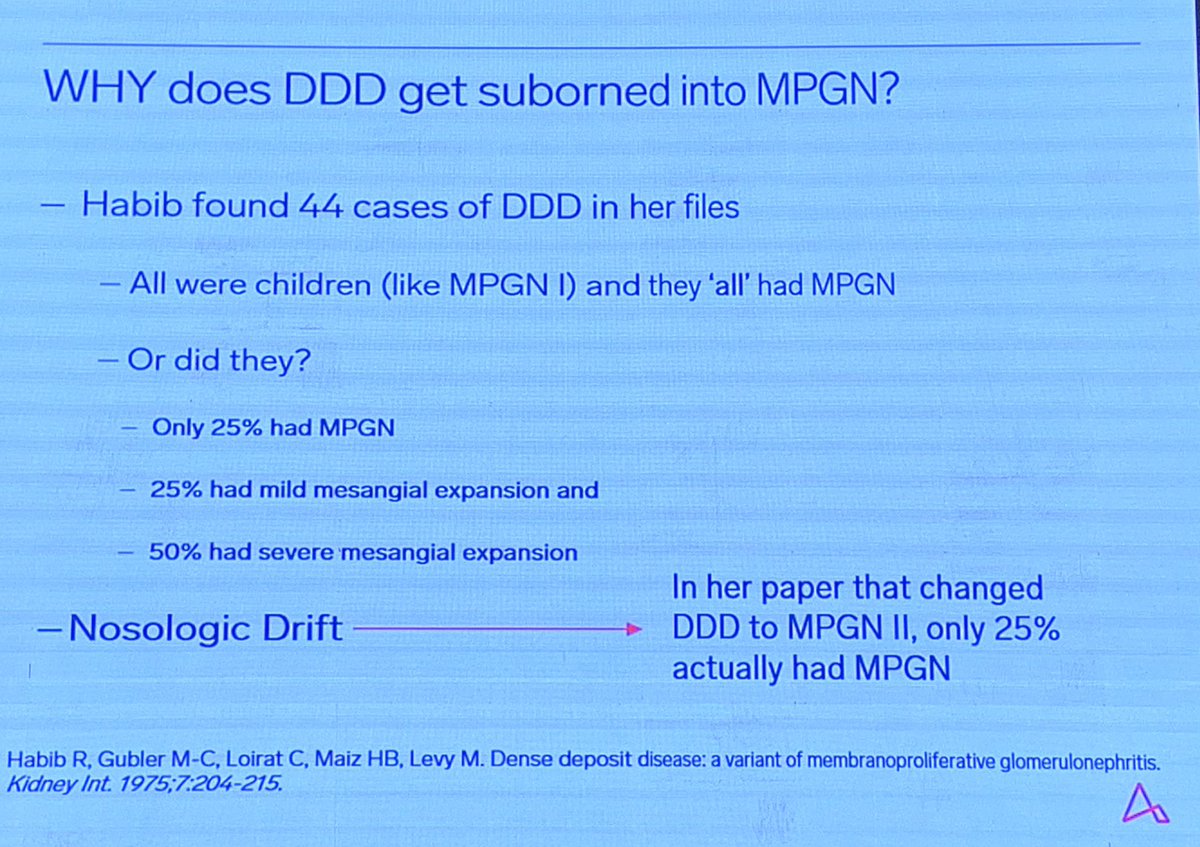
DDD never gets the traction it deserves, rather gets folded into MPGN ll by Dr. Habib’s findings again.
👇🏻 @Kidney_Int
kidney-international.org/article/S0085-…
Difficulty in getting an EM in a disease that’s bonafide rare, probably underlies the missed diagnoses. 7/n
DDD never gets the traction it deserves, rather gets folded into MPGN ll by Dr. Habib’s findings again.
👇🏻 @Kidney_Int
kidney-international.org/article/S0085-…
Difficulty in getting an EM in a disease that’s bonafide rare, probably underlies the missed diagnoses. 7/n
1970s
An MPGN lll type gets ordained as well, with 3 histological subtypes, adding more complexity & layers to a disease still shrouded in mystery. To make matters worse, no treatment is yet deemed satisfactory. 8/n
An MPGN lll type gets ordained as well, with 3 histological subtypes, adding more complexity & layers to a disease still shrouded in mystery. To make matters worse, no treatment is yet deemed satisfactory. 8/n

1980s
More associations are made between possible causative agents and MPGN. But the real ‘operator’ (complement) isn’t given much consideration. 9/n
More associations are made between possible causative agents and MPGN. But the real ‘operator’ (complement) isn’t given much consideration. 9/n
1990s
‘A train wreck’ in the world of MPGN, as Dr. Walker effectively puts it.
Most MPGN l is found to be related to Hepatitis C. Shakes the foundation of all understanding hitherto. 10/n
nejm.org/doi/full/10.10…
‘A train wreck’ in the world of MPGN, as Dr. Walker effectively puts it.
Most MPGN l is found to be related to Hepatitis C. Shakes the foundation of all understanding hitherto. 10/n
nejm.org/doi/full/10.10…

2010
‘Vigorous attempts to identify the underlying mechanisms must be
undertaken whenever the MPGN pattern of injury is found on renal
biopsy.’
⬇️
A pattern, not diagnosis.👍🏻
Thereafter➡️proposal for revised classification in 2011
sciencedirect.com/science/articl…
And newer strides.11/n
‘Vigorous attempts to identify the underlying mechanisms must be
undertaken whenever the MPGN pattern of injury is found on renal
biopsy.’
⬇️
A pattern, not diagnosis.👍🏻
Thereafter➡️proposal for revised classification in 2011
sciencedirect.com/science/articl…
And newer strides.11/n

The above beautifully expounded by Dr. Walker on day 1 of #ApexPathshala 👏🏻
A galvanising delivery in his inimitable style, with many more excellent points not covered here!
(shared with permission)
What a fantastic talk really!
A galvanising delivery in his inimitable style, with many more excellent points not covered here!
(shared with permission)
What a fantastic talk really!

• • •
Missing some Tweet in this thread? You can try to
force a refresh











