HIV has never been proven to be the cause of AIDS.
The AIDS epidemic was iatrogenic.
Pharma leveraged existing illnesses and treated patients with a drug deemed too toxic for cancer patients.
How did this happen?
What can we learn from this?
Thread
The AIDS epidemic was iatrogenic.
Pharma leveraged existing illnesses and treated patients with a drug deemed too toxic for cancer patients.
How did this happen?
What can we learn from this?
Thread
In 1988, Kary Mullis, biochemist and inventor of the PCR test, was working in Santa Monica on nucleic acid analysis for HIV when he realized something: he didn’t have the source paper that proved HIV caused AIDS.
How hard could that be to get?
It would prove impossible.
How hard could that be to get?
It would prove impossible.

As Mullis continually asked colleagues for the elusive reference with no luck, he began to feel uneasy…

Finally, in San Diego, Mullis was face to face with the man himself:
Dr. Luc Montagnier, cofounder of the human immunodeficiency virus (Robert Gallo being the other).
“It would be the last time I would be able to ask my little question without showing anger … So I asked him.”
Dr. Luc Montagnier, cofounder of the human immunodeficiency virus (Robert Gallo being the other).
“It would be the last time I would be able to ask my little question without showing anger … So I asked him.”

Montagnier replied “Why don’t you quote from the CDC Control?”
Mullis pointed out that paper did not show HIV to be the probable cause of AIDS.
Montagnier grew increasingly uncomfortable and looked to his peers for support, but they just watched, curiously.
Mullis pointed out that paper did not show HIV to be the probable cause of AIDS.
Montagnier grew increasingly uncomfortable and looked to his peers for support, but they just watched, curiously.
“Why don’t you quote the work on SIV (Simian Immunodeficiency Virus)?” he asked.
Mullis replied that he read that paper too. What happened to those monkeys didn’t resemble AIDS, and besides, it had only been published recently. “I’m looking for the original paper.”
Mullis replied that he read that paper too. What happened to those monkeys didn’t resemble AIDS, and besides, it had only been published recently. “I’m looking for the original paper.”
Luc Montagnier’s response was to walk away quickly to greet an acquaintance across the room.
Years later, Montagnier would admit Mullis was correct in his criticism.
He would go on to become a pariah in the medical industry.
Years later, Montagnier would admit Mullis was correct in his criticism.
He would go on to become a pariah in the medical industry.
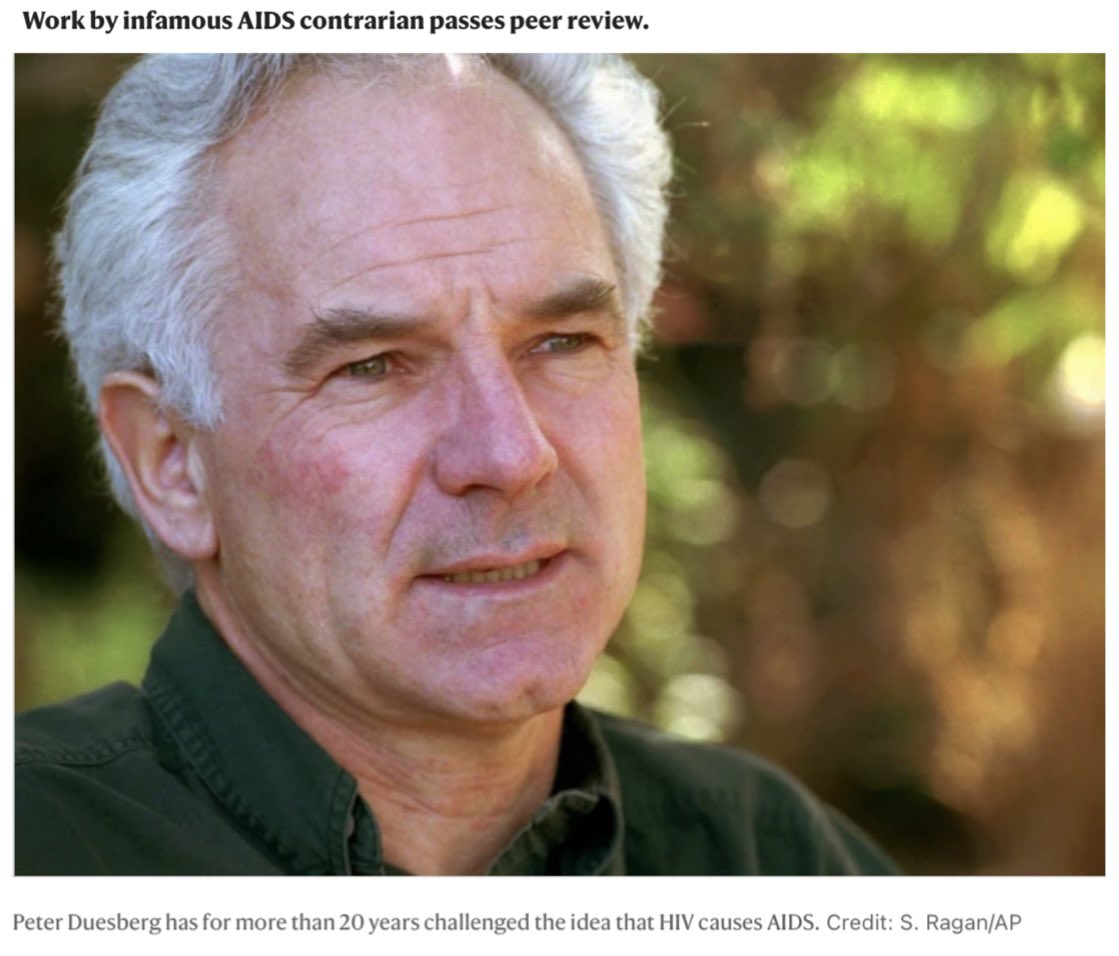
In 1986, molecular biologist—and vocal HIV-AIDS theory critic—Peter Duesberg transferred to the same NIH facility as the other HIV cofounder, Robert Gallo.
Duesberg learned that Gallo’s team was still struggling to find active HIV in the body. His suspicions grew.[1]
Duesberg learned that Gallo’s team was still struggling to find active HIV in the body. His suspicions grew.[1]

Others who joined Duesberg in his criticisms:
Walter Gilbert, biochemist, physicist, pioneer of molecular biology and Nobel laureate
Barbara McClintock, scientist, cytogenecist, and Nobel laureate
Robert Root-Bernstein, professor of physiology, recipient of the “genius grant”
Walter Gilbert, biochemist, physicist, pioneer of molecular biology and Nobel laureate
Barbara McClintock, scientist, cytogenecist, and Nobel laureate
Robert Root-Bernstein, professor of physiology, recipient of the “genius grant”
Kary Mullis protested his own PCR tech being used to detect HIV.
“The HIV test has never been validated,” he said. “It doesn’t show infection; it shows viral particles that may exist in millions of people.”
By the late ‘80s, Mullis was a vocal critic of Fauci and Gallo.
“The HIV test has never been validated,” he said. “It doesn’t show infection; it shows viral particles that may exist in millions of people.”
By the late ‘80s, Mullis was a vocal critic of Fauci and Gallo.
Christine Maggiore adds, “We have a test, but it’s not a test for AIDS; and it’s called an HIV test, but it’s not a test for HIV; and we have a series of problems that we are calling AIDS, but that doesn’t elevate AIDS into a disease.”[2]
Every PCR kit includes a manufacturer’s warning stating “Do not use this kit as the sole basis for detecting viral infection”.
This didn’t keep it from being used for false-positives and subsequent treatments with toxic drugs.
This didn’t keep it from being used for false-positives and subsequent treatments with toxic drugs.
“Despite all the sophisticated biotechnology and vast investment in virology, the best evidence for HIV is only by correlation with antibodies present against it.”
“… however, … a disease is only recorded as AIDS if antibodies to HIV are also found.”[3]
“… however, … a disease is only recorded as AIDS if antibodies to HIV are also found.”[3]

>4,621 diagnosed AIDS cases were HIV-free in 1992.
Those HIV-free AIDS cases were renamed idiopathic CD4-lymphocytopenia (ICL) cases by the CDC and Anthony Fauci[4], a deceptive maneuver that reinforced the correlation.
Those HIV-free AIDS cases were renamed idiopathic CD4-lymphocytopenia (ICL) cases by the CDC and Anthony Fauci[4], a deceptive maneuver that reinforced the correlation.

Latency period for HIV infection has been constantly revised.
It was initially calculated to be 10 months.
By 1996, 10 years or more.
Now? Decades.
Anticipating when a healthy HIV-infected person will present symptoms is impossible for doctors to predict.[5]
It was initially calculated to be 10 months.
By 1996, 10 years or more.
Now? Decades.
Anticipating when a healthy HIV-infected person will present symptoms is impossible for doctors to predict.[5]
“The HIV epidemic is constant and thus old, but the AIDS epidemic is increasing and thus new. Since the two epidemics follow totally different time courses, the HIV epidemic cannot possibly be the cause of the AIDS epidemic.” wrote Duesberg.

According to Farr’s law, infectious diseases spread exponentially, rising and falling more or less symmetrically.
HIV violates this law.
HIV violates this law.


Many HIV positive cases were asymptomatic with a harmless passenger virus.
It’s obvious why treatment with a DNA chain terminator would only make things worse.
HIV is not the virus the media made it out to be.
Koch’s postulates demonstrate this.
It’s obvious why treatment with a DNA chain terminator would only make things worse.
HIV is not the virus the media made it out to be.
Koch’s postulates demonstrate this.

(3) “The cultured microorganism should cause disease when introduced into a healthy organism.”
Western medicine’s understanding of infection disregards terrain theory, yet even within their own germ theory models, HIV fails.
Western medicine’s understanding of infection disregards terrain theory, yet even within their own germ theory models, HIV fails.



“The reports from other labs and biotechnology companies are consistent: HIV grows harmoniously with the cells it infects. The failure to kill T-cells, even under optimal conditions, is the Achilles' heel of the supposed AIDS virus.”[6]

T-cell count can fluctuate 100% on any given day.
In 1993, AIDS cases doubled overnight to include healthy Americans when criteria for what constituted an AIDS diagnosis broadened to include low T-cell count.
The cure? Driving to Canada.
In 1993, AIDS cases doubled overnight to include healthy Americans when criteria for what constituted an AIDS diagnosis broadened to include low T-cell count.
The cure? Driving to Canada.

HIV meets all the criteria for being a passenger virus, and none of the criteria for being the causative, pathogenic virus in AIDS.[7][8]


At a conference in Greensboro, N.C., Dr. Robert Willner was so confident that HIV did not cause AIDS, he injected himself with the blood of an HIV positive man in front of cameras and an audience.
Twice.
He called the AIDS epidemic “the greatest lie ever told”.
Twice.
He called the AIDS epidemic “the greatest lie ever told”.
If AIDS wasn’t the result of a highly contagious virus, then what was it?
An iatrogenic illness and a rebranding of metabolic syndrome.[9]
An iatrogenic illness and a rebranding of metabolic syndrome.[9]


AIDS is an intentionally vague diagnosis.
“Acquired Immune Deficiency Syndrome”
How many illnesses fall under this umbrella?
About 30.
AIDS = pre-existing condition + HIV antibodies
“Acquired Immune Deficiency Syndrome”
How many illnesses fall under this umbrella?
About 30.
AIDS = pre-existing condition + HIV antibodies

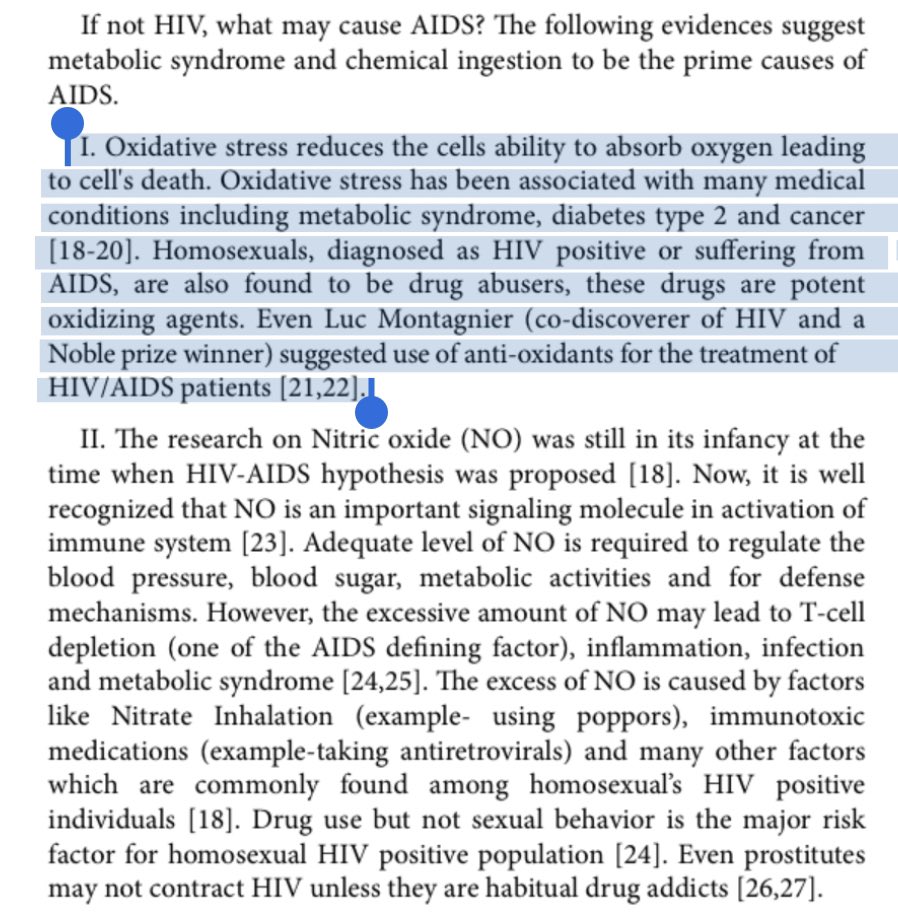
Rampant use of alkyl nitrites, or “poppers”, in the gay community lead to them having high levels of nitric oxide in the body.
Nitric oxide is required for regulation of blood pressure and blood sugar, however, an excess is immunosuppressive[10] and can lead to T-cell depletion.
Nitric oxide is required for regulation of blood pressure and blood sugar, however, an excess is immunosuppressive[10] and can lead to T-cell depletion.

Combined with illicit drug use and immunotoxic antiretrovirals, it’s clear why this group was impacted so severely.
AZT, a drug that would eventually be prescribed to already immunocompromised patients, was itself extremely toxic.
AZT, a drug that would eventually be prescribed to already immunocompromised patients, was itself extremely toxic.

Poppers were a staple in porn shops, bathhouses, bars and nightclubs in the ‘70s.
Floors reeked of intentionally broken bottles.
Bartenders did “last calls” for poppers alongside alcohol.
Consumption of alkyl nitrite in this community was higher than in any other by far.
Floors reeked of intentionally broken bottles.
Bartenders did “last calls” for poppers alongside alcohol.
Consumption of alkyl nitrite in this community was higher than in any other by far.
High nitric oxide means oxidative stress.
Luc Montagnier himself suggested antioxidants as treatment for HIV/AIDS patients.[11][12]
Luc Montagnier himself suggested antioxidants as treatment for HIV/AIDS patients.[11][12]
“Researchers believe poppers to be the direct cause of Kaposi’s sarcoma, a rare form of skin cancer that afflicts the nose, throat, lungs, and skin. Kaposi’s sarcoma was the initial indicator disease of AIDS, but was also common in gay men who were not infected with HIV.”[13]
Chronic illnesses are the varied end results of a handful of the same systems failing (i.e. metabolic syndrome) but allopathic medicine likes to lose the forest for the trees.
The DSM-1, for example, covered about 60 psychological disorders.
DSM-2 lists 182.
DSM-3, 265.
DSM-4 & 5 contain nearly 300.
More obfuscation and condition-labeling means more patented drugs, which means more money for drug companies.
DSM-2 lists 182.
DSM-3, 265.
DSM-4 & 5 contain nearly 300.
More obfuscation and condition-labeling means more patented drugs, which means more money for drug companies.
Which brings us to the highest-paid federal employee, a key figure in the AIDS crisis:
Anthony Fauci.
Since he became director of NIAID in 1984; allergic, autoimmune, and chronic illnesses “mushroomed to afflict 54% of children, up from 12.8% when he took over …”[14]
Anthony Fauci.
Since he became director of NIAID in 1984; allergic, autoimmune, and chronic illnesses “mushroomed to afflict 54% of children, up from 12.8% when he took over …”[14]

“Since Dr. Fauci arrived at NIH, the agency has spent approx. $856 billion.[15][16](2021)
Between 2010 and 2016, every single drug that won approval from the FDA—210 different pharmaceuticals—originated, at least in part, from research funded by the NIH.”[17]
Between 2010 and 2016, every single drug that won approval from the FDA—210 different pharmaceuticals—originated, at least in part, from research funded by the NIH.”[17]

The AIDS epidemic was an overwhelming success for the NIH and a catastrophic failure for anyone unlucky enough to be treated with Fauci’s pet drug, one of the most toxic drugs ever prescribed:
Azidothymidine.
Azidothymidine.

Azidothymidine, “AZT”, Retrovir, or Zidovudine, is a previously shelved drug, considered too toxic and ineffective for cancer patients.
Its side effects mimic a progression of AIDS, blurring the line between disease and treatment.
Of course, only the former was ever blamed.
Its side effects mimic a progression of AIDS, blurring the line between disease and treatment.
Of course, only the former was ever blamed.
AZT was a masterful sleight-of-hand.
An “epidemic” that, while real to certain demographics, became more real as the “antidote” was distributed and patients suffered its effects.
During this, the media whipped the public into a frenzy with constant AIDS fear-mongering.
An “epidemic” that, while real to certain demographics, became more real as the “antidote” was distributed and patients suffered its effects.
During this, the media whipped the public into a frenzy with constant AIDS fear-mongering.

“The public gets most of its information about science from the mass media, and the increasingly concentrated ownership of the media contributes to the use of scientific news as an adjunct to their main business, advertising and product promotion.”[18]
—Dr. Raymond Peat
—Dr. Raymond Peat

At the behest of Burroughs Wellcome (GlaxoSmith-Kline), Fauci’s principal investigators (those in charge of clinical trials & grants) ensured speedy FDA approval—a record 20 months—making AZT available to AIDS patients in 1987 despite evidence of safer and cheaper alternatives.

AZT had already gone through research/trial phases as a failed cancer med, so its revival was highly profitable and convenient for Burroughs Wellcome.
It was never tested on live HIV.
Wellcome did not wish to receive samples from AIDS patients.
It was never tested on live HIV.
Wellcome did not wish to receive samples from AIDS patients.

“Dr. Fauci launched his career by allowing Burroughs Wellcome to charge $10,000 annually (per patient) for AZT,[19] a medication developed exclusively by NIH, and tested and approved by Dr. Fauci himself. Fauci knew the product cost Wellcome a mere $5/dose to manufacture.”[20]
AZT is a “DNA chain terminator”. It destroys DNA synthesis in reproducing cells at random.
AZT works similarly to chemotherapy.
Unlike a course of chemo, AZT was given to patients for years.
AZT works similarly to chemotherapy.
Unlike a course of chemo, AZT was given to patients for years.
AZT’s own developer, Jerome Horwitz, described the drug as “so worthless” that he didn’t think it was even worth patenting.
Horwitz “dumped it on the junk pile” and “didn’t [even] keep the notebooks.”[21]
Horwitz “dumped it on the junk pile” and “didn’t [even] keep the notebooks.”[21]

AZT wasn’t just given to gays, but to the asymptomatic babies of HIV positive mothers.
If the man who cofounded HIV doubted its role in AIDS,
and the man who pioneered the tech to find HIV doubted its validity,
and the drug given to patients was toxic,
what conclusion forms?
If the man who cofounded HIV doubted its role in AIDS,
and the man who pioneered the tech to find HIV doubted its validity,
and the drug given to patients was toxic,
what conclusion forms?
Thanks to an army of principal investigators experienced with finessing regulatory hurdles, Fauci learned how to apply pressure to gain monopoly control.
A link formed between Wellcome, AZT, and the NIH.
After all this time, Fauci still can’t explain how HIV causes AIDS.[22]
A link formed between Wellcome, AZT, and the NIH.
After all this time, Fauci still can’t explain how HIV causes AIDS.[22]

Fauci’s HIV/AIDS drugs have been highly profitable.
In 2000, the market generated about $4 billion
2004, $6.6 billion
2010, $9 billion
By 2020, largely due to repurposing HIV drugs for COVID, it topped $30 billion.[23]
Read that last sentence again.
In 2000, the market generated about $4 billion
2004, $6.6 billion
2010, $9 billion
By 2020, largely due to repurposing HIV drugs for COVID, it topped $30 billion.[23]
Read that last sentence again.


AIDS patients in the US were different than AIDS patients in Africa[24], but the tactics were the same.
Misdiagnosis of various existing illnesses, unreliable antibody testing[25], and iatrogenesis.
Misdiagnosis of various existing illnesses, unreliable antibody testing[25], and iatrogenesis.


As one nurse working in Tanzania put it, "If people die of malaria, it is called AIDS. If they die of herpes, it is called AIDS. I've even seen people die in accidents and it's been attributed to AIDS. The AIDS figures out of Africa are pure lies, pure estimate."[26]
The similarities to COVID tactics and those used in the AIDS crisis are staggering:
• Semantic reclassifications to modify statistics
• Use of PCR to encourage false positives
• Attributing iatrogenic deaths to deaths from the disease…
Nothing changed.
• Semantic reclassifications to modify statistics
• Use of PCR to encourage false positives
• Attributing iatrogenic deaths to deaths from the disease…
Nothing changed.
Despite all the spending and all the hysteria, it’s hard to see the AIDS crisis as anything other than an utter failure.
As we see more adverse events from COVID vaccines, it’s important to remember how the NIH operates.
It continues as long as we allow it to.
As we see more adverse events from COVID vaccines, it’s important to remember how the NIH operates.
It continues as long as we allow it to.

I am not a doctor and none of this is medical advice.

• • •
Missing some Tweet in this thread? You can try to
force a refresh