"We've got parents with chronic health conditions..." Clancy Clonnal from @SHSorguk.
Who'd have thought that the consequences of constant high Covid infections would fall hardest on those most at risk?
Clinically Vulnerable Families have been struggling @NickMartinSKY.
1/
Who'd have thought that the consequences of constant high Covid infections would fall hardest on those most at risk?
Clinically Vulnerable Families have been struggling @NickMartinSKY.
1/
https://twitter.com/SkyNews/status/1659561106317213701
Unfortunately, time and again, our needs have not been considered.
Clinically Vulnerable people have a 5.4x increased risk of Long Covid and an 8.5x increased risk of death (data from the final ONS Covid survey).
Withdrawing protections from schools has hit us hardest.
2/
Clinically Vulnerable people have a 5.4x increased risk of Long Covid and an 8.5x increased risk of death (data from the final ONS Covid survey).
Withdrawing protections from schools has hit us hardest.
2/

Our increased risks, without any protections in place, make our lives more difficult and impact our children - even if they are attending school. It is a barrier to attendance and a barrier to learning.
3/
3/

Many Clinically Vulnerable Families no longer feature in official attendance data, as they have been off-rolled, because schools and local authorities do not want their own data blighted.
4/
4/

Clinically Vulnerable Families reject the incredibly distasteful title "Ghost Children".
This article by @samanthajbooth explains in more detail:
5/
schoolsweek.co.uk/dont-call-us-g…
This article by @samanthajbooth explains in more detail:
5/
schoolsweek.co.uk/dont-call-us-g…
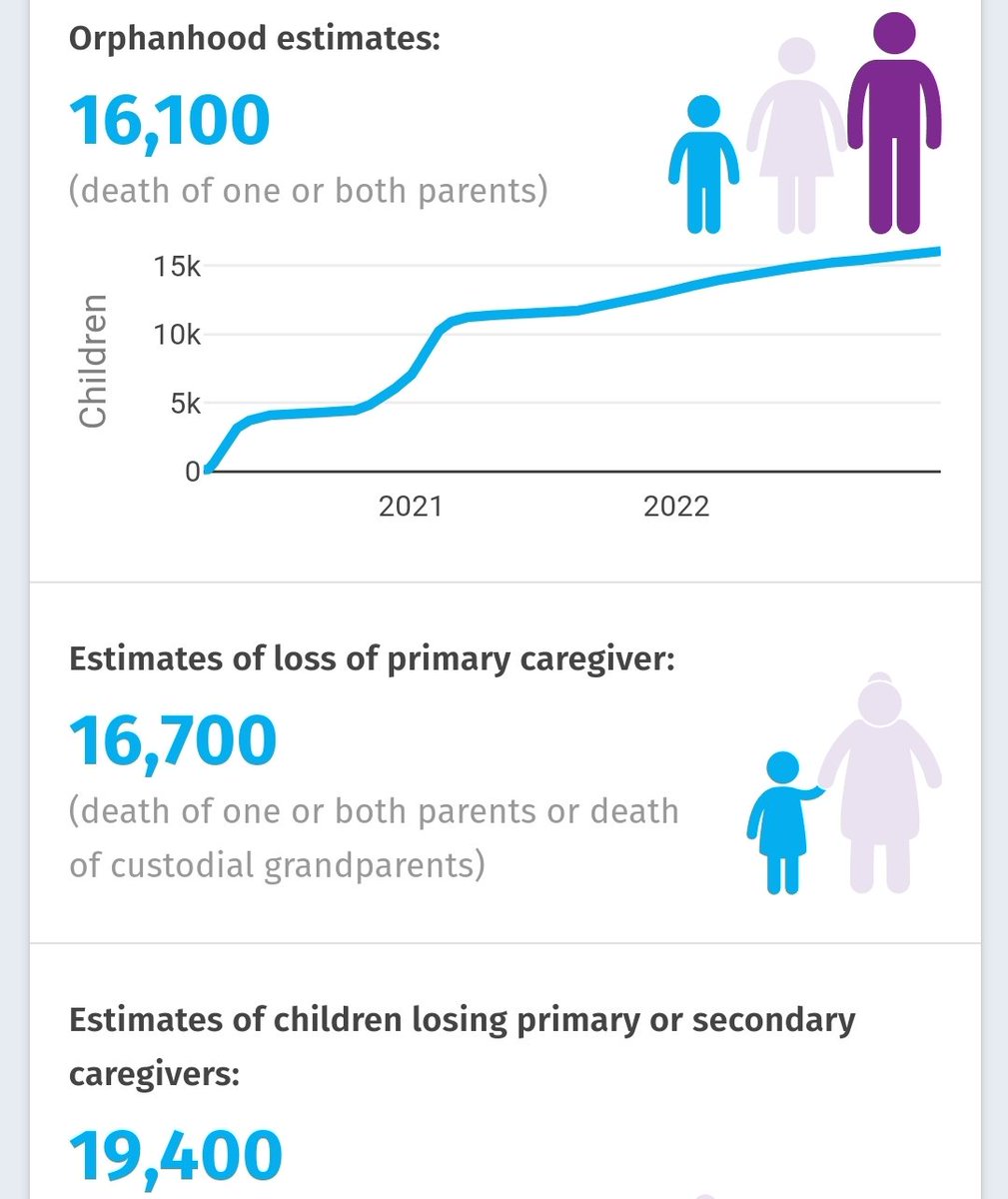
Minimum estimates for Covid Orphans continue to grow.
Because by not protecting our children were are not protecting their households, families and communities.
6/
Because by not protecting our children were are not protecting their households, families and communities.
6/
We have been collecting data,
We hope to share it with the Education Committee Inquiry into attendance, but we have yet to be invited to share our oral evidence.
Even winter pressures on healthcare affected our school attendance.
7/
We hope to share it with the Education Committee Inquiry into attendance, but we have yet to be invited to share our oral evidence.
Even winter pressures on healthcare affected our school attendance.
7/

All children are now frequently getting sick with Covid itself, as it remains in high prevalence year-round. This also has a direct impact on attendance figures.
Whilst some people may be asymptomatic, others can take a long time to recover - if they ever do...
8/
Whilst some people may be asymptomatic, others can take a long time to recover - if they ever do...
8/

Children are developing post-viral conditions such as T1 diabetes which make them Clinically Vulnerable.
And highly vulnerable children are now locked out of high demand special schools due to a shortfall in provision.
However, there is something they could do...
9/
And highly vulnerable children are now locked out of high demand special schools due to a shortfall in provision.
However, there is something they could do...
9/

And it isn't recycling the old "Schools Bill" to crack down harder on struggling parents.
Because fines, prosecutions, social services referrals, and school attendance orders are blunt instruments, which only make matters worse and won't fix our problem.
10/
Because fines, prosecutions, social services referrals, and school attendance orders are blunt instruments, which only make matters worse and won't fix our problem.
10/

All we are asking for is a safe learning environment. It is a very simple and basic request.
Because even those who are in school are struggling. How can children learn or perform when 'personal responsibility' means that they are constantly managing risk?
11/
Because even those who are in school are struggling. How can children learn or perform when 'personal responsibility' means that they are constantly managing risk?
11/

💙 We want to *live* with Covid
💜 #educationANDlives are essentials
💗 Everyone needs safe schools
Let's invest in health. Air filtration can reduce the risks for everyone.
By reducing Covid, 'flu, Strep A. & RSV we improve pupil & staff attendance and community health.
12/
💜 #educationANDlives are essentials
💗 Everyone needs safe schools
Let's invest in health. Air filtration can reduce the risks for everyone.
By reducing Covid, 'flu, Strep A. & RSV we improve pupil & staff attendance and community health.
12/

Join us in the unmentionable place to find the most supportive community and to contribute to our attendance survey:
Search for : Clinically Vulnerable Families
Search for : Clinically Vulnerable Families

Additionally, please complete the DfE survey requesting evidence on children missing from education.
⬇️⬇️⬇️
consult.education.gov.uk/vulnerable-chi…
⬆️⬆️⬆️
14/
⬇️⬇️⬇️
consult.education.gov.uk/vulnerable-chi…
⬆️⬆️⬆️
14/
https://twitter.com/LongCovidKids/status/1659827897681551360?t=dmjsBOA6tA5fgrcjukdubQ&s=19
• • •
Missing some Tweet in this thread? You can try to
force a refresh