Intro:
-true oncological emergency❗️
-up to 6% of cancer patients
-annual incidence of hospitalizations secondary to MSCC among patients with advanced cancer ~3.5%
-multiple myeloma and non-Hodgkin lymphoma with highest cancer-specific incidence
-prognosis poor
2/11
-true oncological emergency❗️
-up to 6% of cancer patients
-annual incidence of hospitalizations secondary to MSCC among patients with advanced cancer ~3.5%
-multiple myeloma and non-Hodgkin lymphoma with highest cancer-specific incidence
-prognosis poor
2/11

Definition of MSCC:
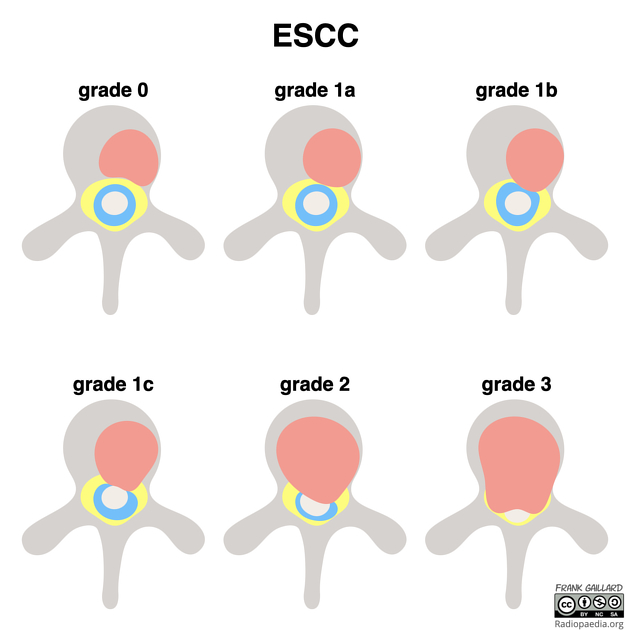
-any radiologic evidence of indentation of the thecal sac or spinal cord compression, whether or not there are neurologic signs and symptoms associated with compression
-grading using the "epidural spinal cord compression (ESCC) scale" (Bilsky scale)
3/11
-any radiologic evidence of indentation of the thecal sac or spinal cord compression, whether or not there are neurologic signs and symptoms associated with compression
-grading using the "epidural spinal cord compression (ESCC) scale" (Bilsky scale)
3/11
Pathophysiology:
-mostly due to metastases to vertebral bodies
👉erode into spinal canal & encroach on spinal cord
-paravertebral tumors can extend through neural foramina 👉cord compression
-intramedullary & meningeal rare
-Most locations: thoracic>lumbar>cervical spine
4/11
-mostly due to metastases to vertebral bodies
👉erode into spinal canal & encroach on spinal cord
-paravertebral tumors can extend through neural foramina 👉cord compression
-intramedullary & meningeal rare
-Most locations: thoracic>lumbar>cervical spine
4/11

Clinic:
-back pain
-paralysis, sensory loss, bladder and bowel dysfunction can evolve rapidly
-Cauda equina syndrome👉compression in lumbosacral spine
-20% do not have a known cancer diagnosis at the time the MSCC is diagnosed❗️
-know your dermatomes❗️
5/11
-back pain
-paralysis, sensory loss, bladder and bowel dysfunction can evolve rapidly
-Cauda equina syndrome👉compression in lumbosacral spine
-20% do not have a known cancer diagnosis at the time the MSCC is diagnosed❗️
-know your dermatomes❗️
5/11

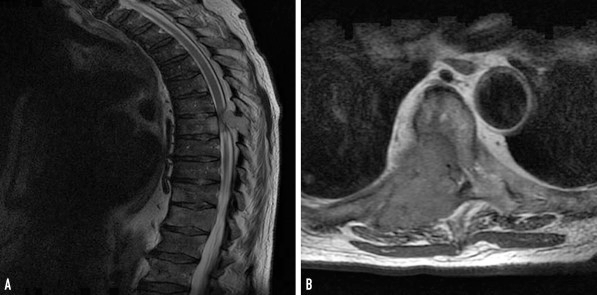
Diagnosis:
-method of choice is MRI
-if possible, important to image ENTIRE spine because up to 40% have multiple levels of compression or cord impingement
-CT, with or without myelography, if MRI is contraindicated or not available
-assess ESCC and instability
6/11
-method of choice is MRI
-if possible, important to image ENTIRE spine because up to 40% have multiple levels of compression or cord impingement
-CT, with or without myelography, if MRI is contraindicated or not available
-assess ESCC and instability
6/11
Differential of MSCC:
-degeneration
-abscess
-fracture
-Vascular malformation
-epidural hematoma
-extramedullary hematopoiesis
-systemic inflammatory disease
7/11
-degeneration
-abscess
-fracture
-Vascular malformation
-epidural hematoma
-extramedullary hematopoiesis
-systemic inflammatory disease
7/11

Treatment:
-initiate without delay
-assess motor function before
-consider high-dose dexamethasone for severe deficits in whom small potential gain may outweigh the risks
-almost all patients should be evaluated urgently for a decompressive surgical procedure
8/11
-initiate without delay
-assess motor function before
-consider high-dose dexamethasone for severe deficits in whom small potential gain may outweigh the risks
-almost all patients should be evaluated urgently for a decompressive surgical procedure
8/11
Radiation:
-most patients, whether or not get decompressive surgery
-conventional external beam radiation therapy (cEBRT)
👉~70% pain improvement, 50% without instability with resolution
👉variety of schedules: single (8 Gy), protracted (30-40 Gy in 10-20 fractions)
9/11
-most patients, whether or not get decompressive surgery
-conventional external beam radiation therapy (cEBRT)
👉~70% pain improvement, 50% without instability with resolution
👉variety of schedules: single (8 Gy), protracted (30-40 Gy in 10-20 fractions)
9/11

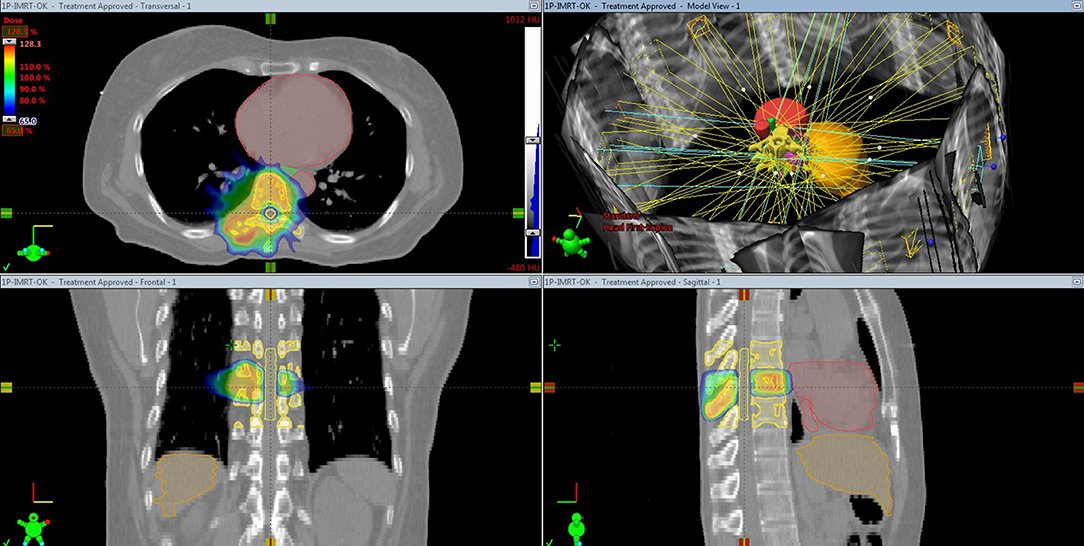
Stereotactic body radiotherapy (SBRT):
-cEBRT limited by proximity of spinal cord
-SBRT with precisely targeted high dose to tumor (even separated by 2 to 3 millimeters from spinal cord)
BUT
-less useful for relatively radioresistant tumors
10/11
-cEBRT limited by proximity of spinal cord
-SBRT with precisely targeted high dose to tumor (even separated by 2 to 3 millimeters from spinal cord)
BUT
-less useful for relatively radioresistant tumors
10/11
Summary for MSCC:
❗️Emergency
❗️Myeloma & non-Hodgkin lymphoma
❗️Thoracic>lumbar>cervical
❗️Pain, sensory & motor dysfunction, in ~40% first sign even before cancer diagnosis
❗️scales: ESCC & instability score
❗️MRI
❗️Treat immediately: dexamethasone, surgery +/- radiation
❗️Emergency
❗️Myeloma & non-Hodgkin lymphoma
❗️Thoracic>lumbar>cervical
❗️Pain, sensory & motor dysfunction, in ~40% first sign even before cancer diagnosis
❗️scales: ESCC & instability score
❗️MRI
❗️Treat immediately: dexamethasone, surgery +/- radiation
References & resources:
mayoclinicproceedings.org/article/S0025-…
frontiersin.org/articles/10.33…
ashpublications.org/blood/article/…
pubmed.ncbi.nlm.nih.gov/27488300/
mayoclinicproceedings.org/article/S0025-…
frontiersin.org/articles/10.33…
ashpublications.org/blood/article/…
pubmed.ncbi.nlm.nih.gov/27488300/
• • •
Missing some Tweet in this thread? You can try to
force a refresh