#ASCO23 Tweetorial on putting results of PEACE-1 in context. Here we go!
@ASCO @ASTRO_org @HimanshuNagarMD @DrRanaMcKay @AlbertoBossial @Prof_Nick_James @PCaParker
@ASCO @ASTRO_org @HimanshuNagarMD @DrRanaMcKay @AlbertoBossial @Prof_Nick_James @PCaParker
1/n
ADT + tx intensification w/ chemo or ARSI is SOC based on lots of RCTs
No OS diff seen in STAMPEDE from ADT+Abi vs ADT+doce (FFS difference as ARSI suppress PSA = FFS).
No clear role of triplet therapy in low volume (ARASENS)
Thus, SOC is ADT+doce or ARSI for low volume
ADT + tx intensification w/ chemo or ARSI is SOC based on lots of RCTs
No OS diff seen in STAMPEDE from ADT+Abi vs ADT+doce (FFS difference as ARSI suppress PSA = FFS).
No clear role of triplet therapy in low volume (ARASENS)
Thus, SOC is ADT+doce or ARSI for low volume

2/n
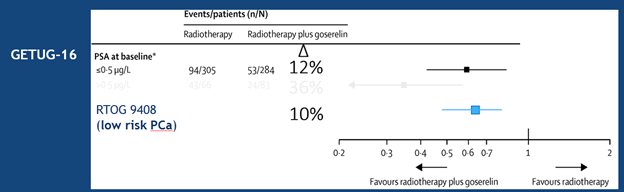
RT to primary for low volume improved FFS and OS in STAMPEDE arm H, and in IPD meta-analysis w/ HORRAD RCT.
18% of men received ADT+doce on STAMPEDE arm H, and no interaction of differential effect noticed.
Thus, ADT+doce+RT in low volume was the SOC at this point.
RT to primary for low volume improved FFS and OS in STAMPEDE arm H, and in IPD meta-analysis w/ HORRAD RCT.
18% of men received ADT+doce on STAMPEDE arm H, and no interaction of differential effect noticed.
Thus, ADT+doce+RT in low volume was the SOC at this point.

3/n
In countries like US majority use an ARSI instead of doce, esp in low volume.
Given doce and abi have similar long-term OS (post-hoc in STAMPEDE), and recent data in cN1 disease shows RT+ADT +/- Abi, that Abi improves OS, many adopted RT+ADT+RT to primary.
@AttardLab
In countries like US majority use an ARSI instead of doce, esp in low volume.
Given doce and abi have similar long-term OS (post-hoc in STAMPEDE), and recent data in cN1 disease shows RT+ADT +/- Abi, that Abi improves OS, many adopted RT+ADT+RT to primary.
@AttardLab

4/n
Now, some argued that we have no clean trial of ADT+RT +/- Abi, or ADT+Abi +/- RT.
However, if one were to add only 1 therapy to ADT it is undeniable that the value based option would be RT to the primary and not Abi.
Thus, SOC is ADT+RT +/- tx intensification at this point
Now, some argued that we have no clean trial of ADT+RT +/- Abi, or ADT+Abi +/- RT.
However, if one were to add only 1 therapy to ADT it is undeniable that the value based option would be RT to the primary and not Abi.
Thus, SOC is ADT+RT +/- tx intensification at this point

5/n
Here is where PEACE-1 comes in.
Only in hindsight we know know it would need to be 2-3 times the size to answer all the questions it sought out to if the co-primary endpoints were truly to include rPFS and OS.
This is because of the introduction of doce into the SOC arms
Here is where PEACE-1 comes in.
Only in hindsight we know know it would need to be 2-3 times the size to answer all the questions it sought out to if the co-primary endpoints were truly to include rPFS and OS.
This is because of the introduction of doce into the SOC arms

6/n
PEACE-1 enrolled 1173 men.
-43% were low volume = 505 men
-50% of low volume got doce
-About half of these got ADT alone and not ADT+Abi
Thus, only ~125 men were randomized to ADT+Abi +/- RT for low volume!
STAMPEDE arm H low volume ~1000 men!
PEACE-1 enrolled 1173 men.
-43% were low volume = 505 men
-50% of low volume got doce
-About half of these got ADT alone and not ADT+Abi
Thus, only ~125 men were randomized to ADT+Abi +/- RT for low volume!
STAMPEDE arm H low volume ~1000 men!
7/n
Thus, the trial turned out testing triplet systemic therapy, which already reviewed not needed in low volume and adds even more cost and toxicity.
Despite this, RT to primary on top of excessive systemic tx improve rPFS!!!
Thus, the trial turned out testing triplet systemic therapy, which already reviewed not needed in low volume and adds even more cost and toxicity.
Despite this, RT to primary on top of excessive systemic tx improve rPFS!!!


8/n
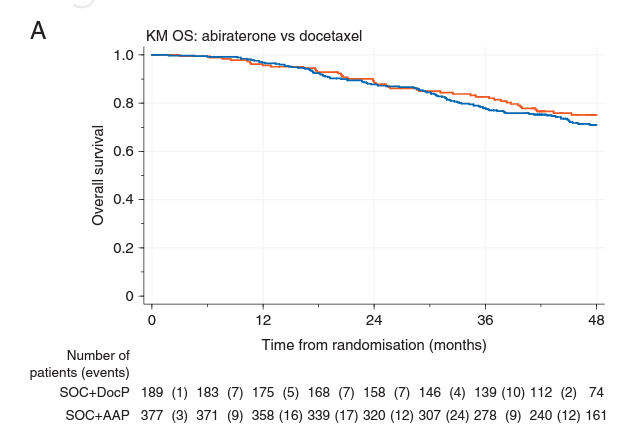
And as noted on it is underpowered for OS for low volume, it still showed important trends:
1. OS for SOC+RT was numerically superior to SOC+Abi (STAMPEDE predicted RT and abi have similar HR of benefit)
2. SOC+Abi+RT had numerically best OS but subsets are tiny
And as noted on it is underpowered for OS for low volume, it still showed important trends:
1. OS for SOC+RT was numerically superior to SOC+Abi (STAMPEDE predicted RT and abi have similar HR of benefit)
2. SOC+Abi+RT had numerically best OS but subsets are tiny


• • •
Missing some Tweet in this thread? You can try to
force a refresh