Dr. Rancourt PhD: "There's a strong correlation to poverty, which is one of the pieces of evidence that allows you to say that this is not a virus. [..] No matter how you slice it, there's absolutely no correlation with age, which is a definitive proof that this cannot be COVID"
"During the covid period, all western countries cut antibiotics prescriptions by 50%, so they were not treating bacterial pneumonia."
"The age structure of the excess mortality has changed as you move into the vaccination period."
"The age structure of the excess mortality has changed as you move into the vaccination period."
"These peaks occur in very specific hotspots, but synchronously around the world [..] that from an epidemiological standpoint is strictly impossible, because the time from seeding of an infection to the sudden rise of mortality is completely uncertain."
"The virus absolutely refused to cross these borders, of course this is absurd, a viral respiratory disease is believed to spread, and it does not need a passport, and it does not respect borders, so that's yet another proof, that this is not a viral respiratory pandemic."
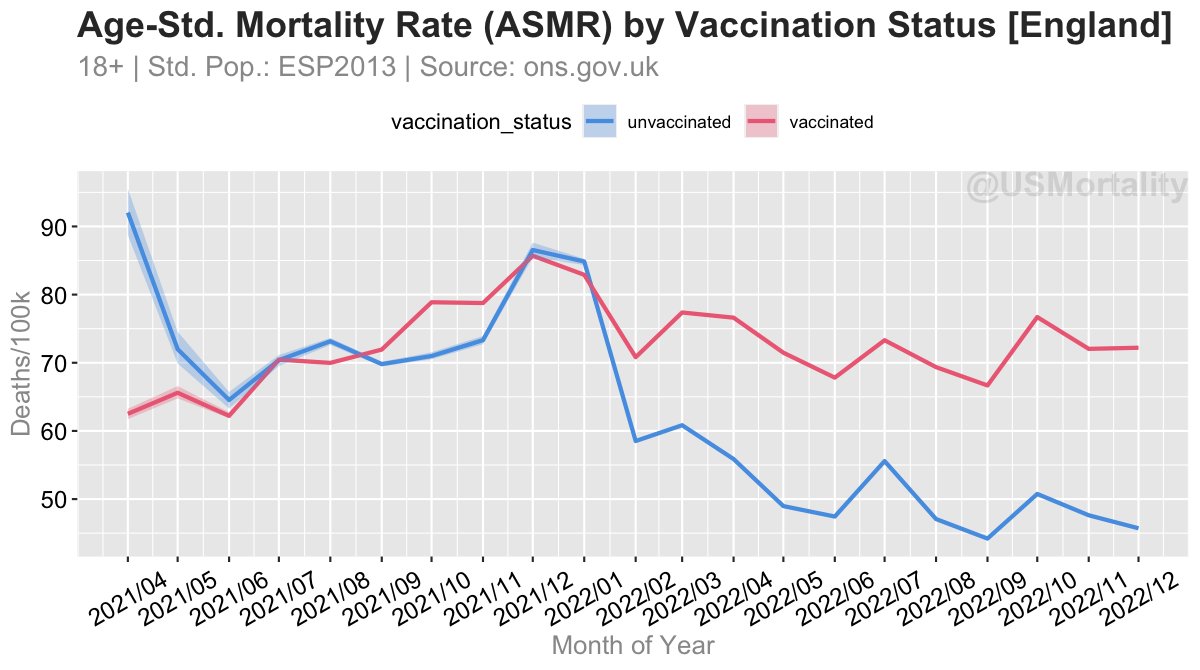
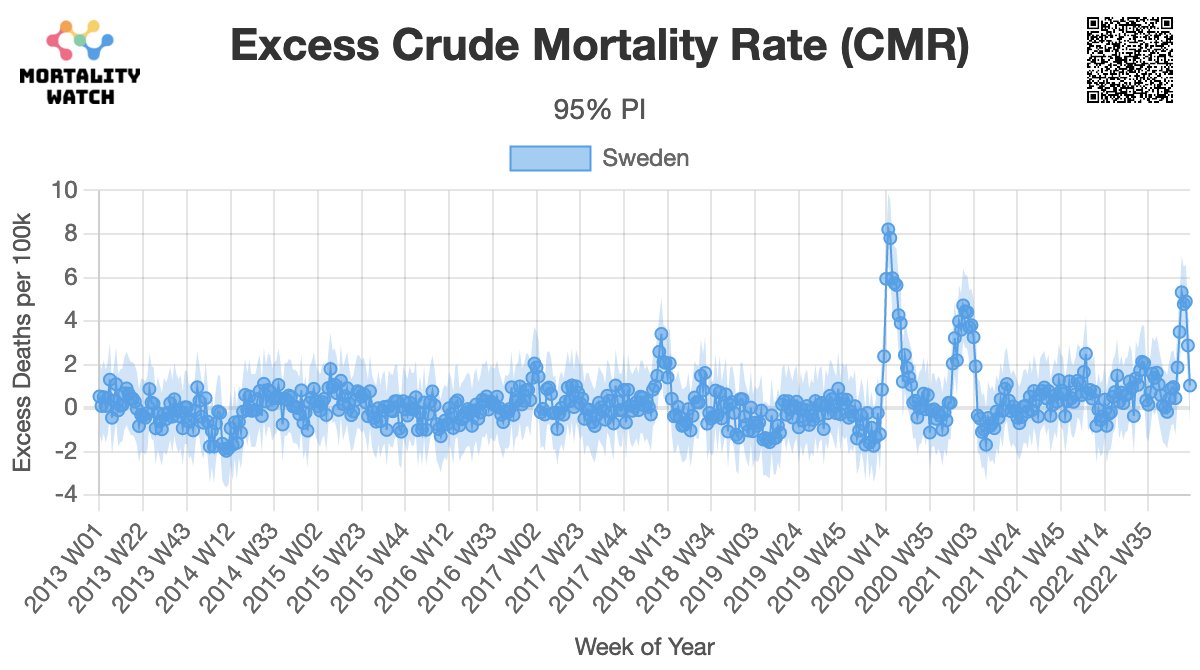
"You see, as a consequence of the vaccine rollout, there's a higher regime of mortality."
"Same thing for each of the states in Australia."
"The large peak [in the southern US] coincides with [the] vaccine equity [program]"
"Same thing for each of the states in Australia."
"The large peak [in the southern US] coincides with [the] vaccine equity [program]"
"You are injecting people, that are at high risk of dying when you inject the elderly"
"Young adults, are above the exponential [risk]. There's a plateau of risk of dying for young adults."
"Young adults, are above the exponential [risk]. There's a plateau of risk of dying for young adults."
And finally, Dr. Rancourt's conclusions:
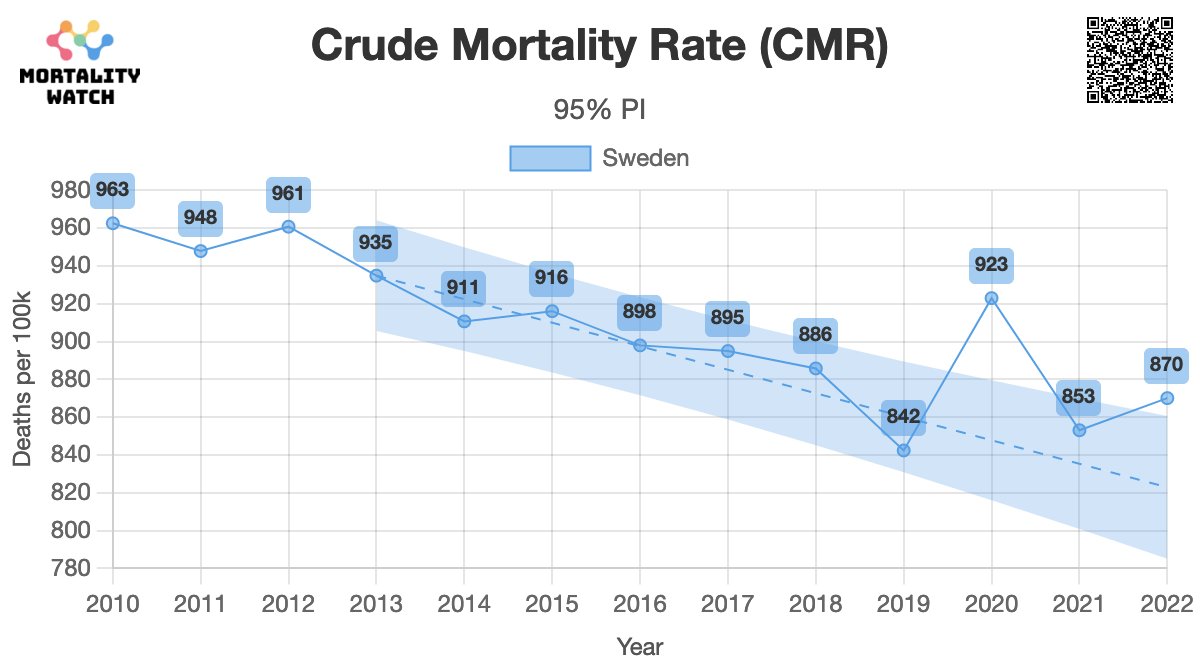
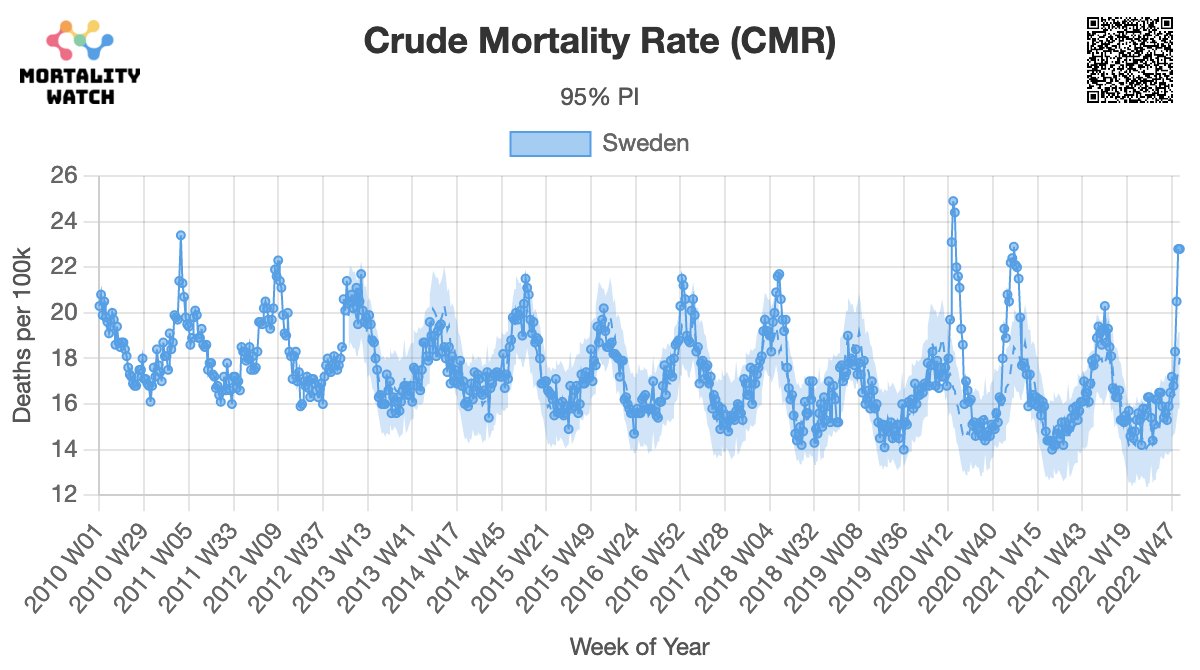
1) If govt's had done nothing - no excess mortality. There was no pandemic, that caused excess mortality.
2) The measures that governments applied, caused excess mortality.
3) The vaccination campaign definitely caused excess mortality.
1) If govt's had done nothing - no excess mortality. There was no pandemic, that caused excess mortality.
2) The measures that governments applied, caused excess mortality.
3) The vaccination campaign definitely caused excess mortality.
And finally, please follow Dr. Rancourt himself: @denisrancourt
Watch the full video: rumble.com/v2ohtte-physic…
Find all my latest work: mortality.watch
Watch the full video: rumble.com/v2ohtte-physic…
Find all my latest work: mortality.watch
• • •
Missing some Tweet in this thread? You can try to
force a refresh