
🇺🇸🇪🇺 Software Engineer • COVID-19 Research, Bioinformatics & Statistics • https://t.co/VUPbRbRjx3
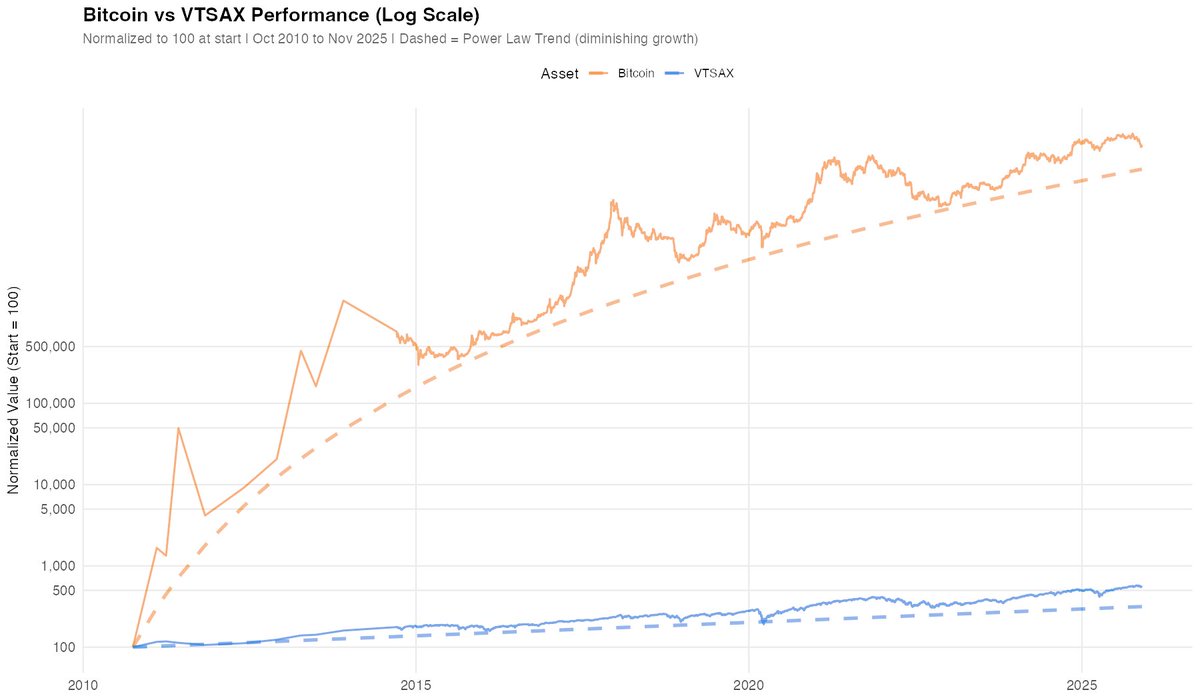 Bitcoin follows a "power law" - returns diminish over time.
Bitcoin follows a "power law" - returns diminish over time.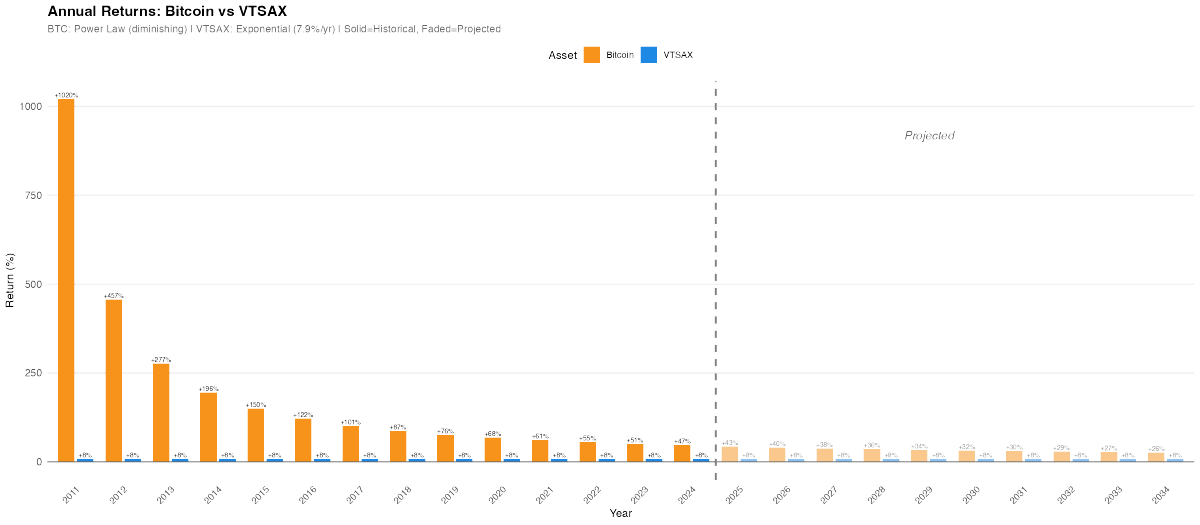
 76% of deaths have UNKNOWN vaccination status.
76% of deaths have UNKNOWN vaccination status.
 Negative controls—where identical methodology is applied to samples without the target virus—are essential for validating results. Instead, they relied solely on unvalidated PCR testing to confirm assumed presence prior to sequencing.
Negative controls—where identical methodology is applied to samples without the target virus—are essential for validating results. Instead, they relied solely on unvalidated PCR testing to confirm assumed presence prior to sequencing.
 This strikes at the core of today’s vaccination debate. Even if we accept—despite questionable evidence, such as the lack of decline among Asian populations—that there has been a reduction, it amounts to just 1.5 fewer cervical cancer deaths per million white females..
This strikes at the core of today’s vaccination debate. Even if we accept—despite questionable evidence, such as the lack of decline among Asian populations—that there has been a reduction, it amounts to just 1.5 fewer cervical cancer deaths per million white females..
 ... by Enders et al. in 1963, measles deaths had already declined by 97.2%, from 12,992 in 1919 to 364 in 1963—without vaccination. While deaths dropped to typically less than 10/year.
... by Enders et al. in 1963, measles deaths had already declined by 97.2%, from 12,992 in 1919 to 364 in 1963—without vaccination. While deaths dropped to typically less than 10/year.


 So here are the chart with the highest precision.
So here are the chart with the highest precision. 
 Evaluating the safety and effectiveness of vaccines requires careful scrutiny of clinical trial methodologies. Here are five essential steps to identify potential flaws or fraud in vaccine studies.
Evaluating the safety and effectiveness of vaccines requires careful scrutiny of clinical trial methodologies. Here are five essential steps to identify potential flaws or fraud in vaccine studies.
 The response:
The response: Instead, people like Dr. Binder have pointed out since 2020, that the use of mass PCR testing, is entirely responsible for this phenomenon:
Instead, people like Dr. Binder have pointed out since 2020, that the use of mass PCR testing, is entirely responsible for this phenomenon: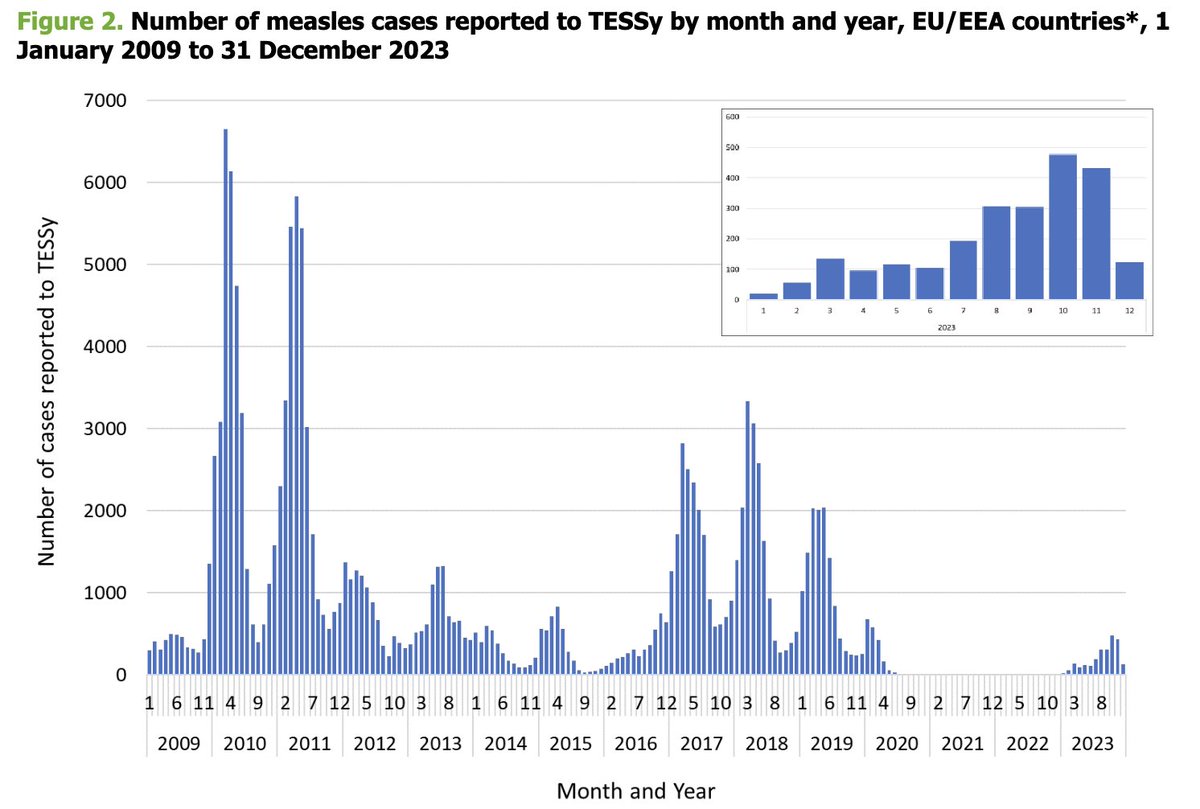 ecdc.europa.eu/sites/default/…
ecdc.europa.eu/sites/default/…
 ... and a logistic growth function to simulate placebo vaccination from 0 to 75% of the population.
... and a logistic growth function to simulate placebo vaccination from 0 to 75% of the population.
 The initial peak may be related to confounding as more elderly/frail were prioritized, to reporting artifact (Fenton et al.), or vaccine harm.
The initial peak may be related to confounding as more elderly/frail were prioritized, to reporting artifact (Fenton et al.), or vaccine harm. I have analyzed the official NZ data which was published due to a FOIA, and initially analyzed by @sco0psmcgoo.
I have analyzed the official NZ data which was published due to a FOIA, and initially analyzed by @sco0psmcgoo.
 Moreover, they did not even bother to test for potential of these vaccines to cause cancer or mutations.
Moreover, they did not even bother to test for potential of these vaccines to cause cancer or mutations.
 Same chart with 95% prediction intervals.
Same chart with 95% prediction intervals. 
 This is not based on any y-axis trickery either.
This is not based on any y-axis trickery either. 
 Excess Mortality:
Excess Mortality: 
 However, that's completely de-confounded or masked when using ASMR - which would suggest, that it's mostly elderly that are dying?
However, that's completely de-confounded or masked when using ASMR - which would suggest, that it's mostly elderly that are dying? 



 Again noteworthy, due to the average baseline method, the increase is not due to a modeling artifact!
Again noteworthy, due to the average baseline method, the increase is not due to a modeling artifact!