
An important teaching case
A 45 year old lady with significant vascular risk factors presented with hyperacute onset dimness in the L side of her field of vision, specially in the bottom half.
There is no other significant neurological or systemic hx.
A 45 year old lady with significant vascular risk factors presented with hyperacute onset dimness in the L side of her field of vision, specially in the bottom half.
There is no other significant neurological or systemic hx.
Clinical examination revealed only a BP - 150/90, R arm, sitting position with confrontation perimetry showing an incongruent, incomplete L sided homonymous hemianopia.
A homonymous hemianopia localizes posterior to the optic chiasma where the nasal hemiretinal fibers decussate.
A L sided HH localizes a lesion to the R post-chiasmatic visual pathway.
Incongruency argues for a relatively anterior localization of the lesion ie away from cortex.
A L sided HH localizes a lesion to the R post-chiasmatic visual pathway.
Incongruency argues for a relatively anterior localization of the lesion ie away from cortex.
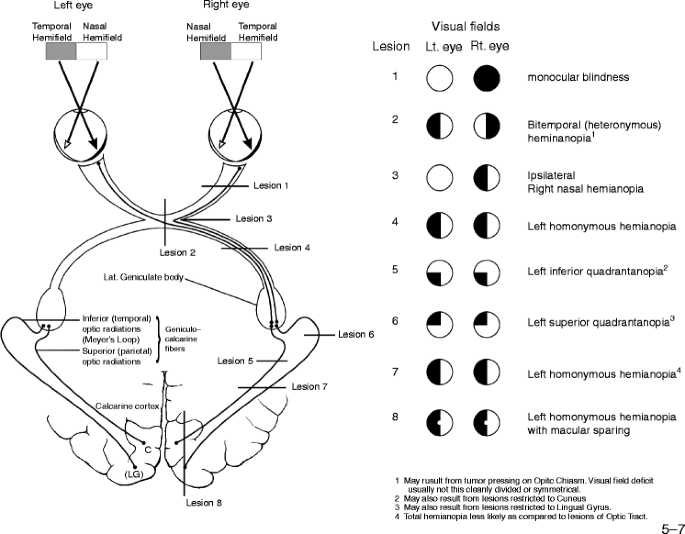
As expected, neuroimaging reveals a lesion in the R optic radiations.

This is likely an infarct, as evidenced by the hyperacuity of the insult.
But she has no vascular risk factors and the insult is maximal at onset.
This argues for an embolic etiology.
But she has no vascular risk factors and the insult is maximal at onset.
This argues for an embolic etiology.
If its embolic without significant vascular risk factors, we must think of cardioembolism.
So we have to go back to the patient again --> a more detailed CVS exam reveals the classic mid-diastolic rumbling murmur of a mitral stenosis without any irregular pulse.
So we have to go back to the patient again --> a more detailed CVS exam reveals the classic mid-diastolic rumbling murmur of a mitral stenosis without any irregular pulse.
Echocardiography confirms the diagnosis of severe MS with MVA of 0.8 sq. cm (by planimetry).
A 12 lead ECG doesn't reveal any AF. Holter has been planned.
A 12 lead ECG doesn't reveal any AF. Holter has been planned.
We have started the patient on a VKA, as per present guidelines and referred them to our cardiology colleagues for further management.
Any teaching points you wish to add?
Please post in the comments below!
#MedTwitter
#neurotwitter
#mitralstenosis
#stroke
#cardioembolism
Please post in the comments below!
#MedTwitter
#neurotwitter
#mitralstenosis
#stroke
#cardioembolism
*no significant vascular risk factors.
• • •
Missing some Tweet in this thread? You can try to
force a refresh





