How common are chronic SARS-CoV-2 infections?
I think that at least 1 in 1,000 infections lead to long term (>4 month) chronic infection.
This is how I came up with that number.
1/
I think that at least 1 in 1,000 infections lead to long term (>4 month) chronic infection.
This is how I came up with that number.
1/
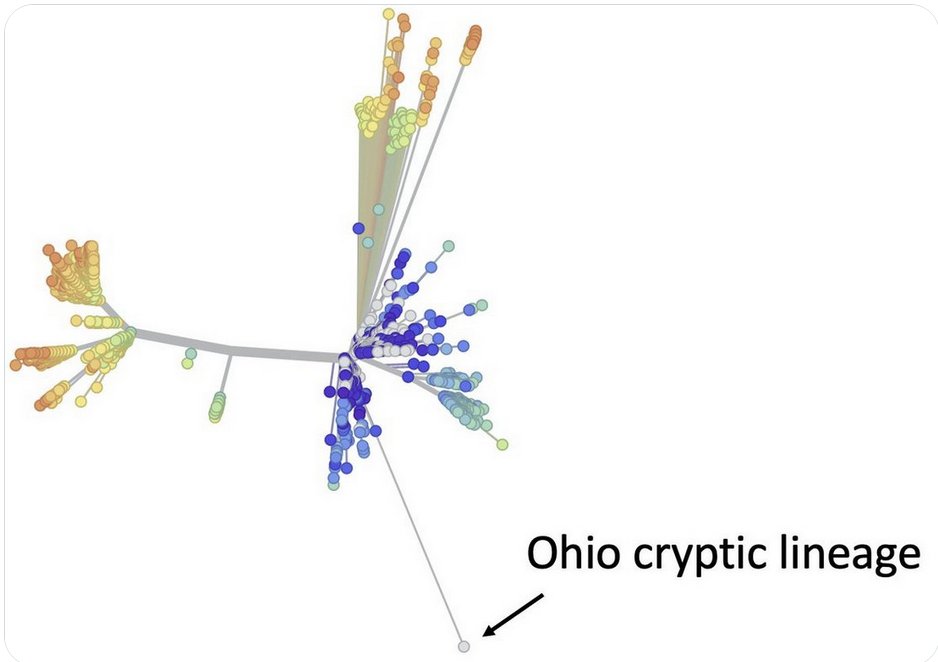
I’ve mentioned before, the mutation Orf1a:K1795Q appears very frequently in very advanced chronic infections and cryptic lineages.
I’ve tried to use the frequency of this mutation to make estimates of how frequent chronic infections are.
2/
I’ve tried to use the frequency of this mutation to make estimates of how frequent chronic infections are.
2/
https://twitter.com/SolidEvidence/status/1672708504572907526
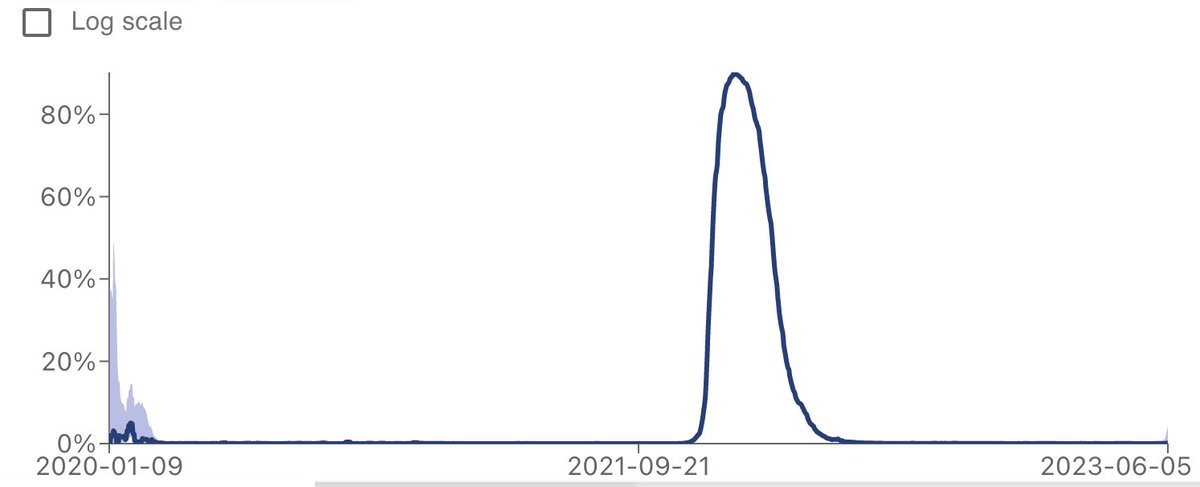
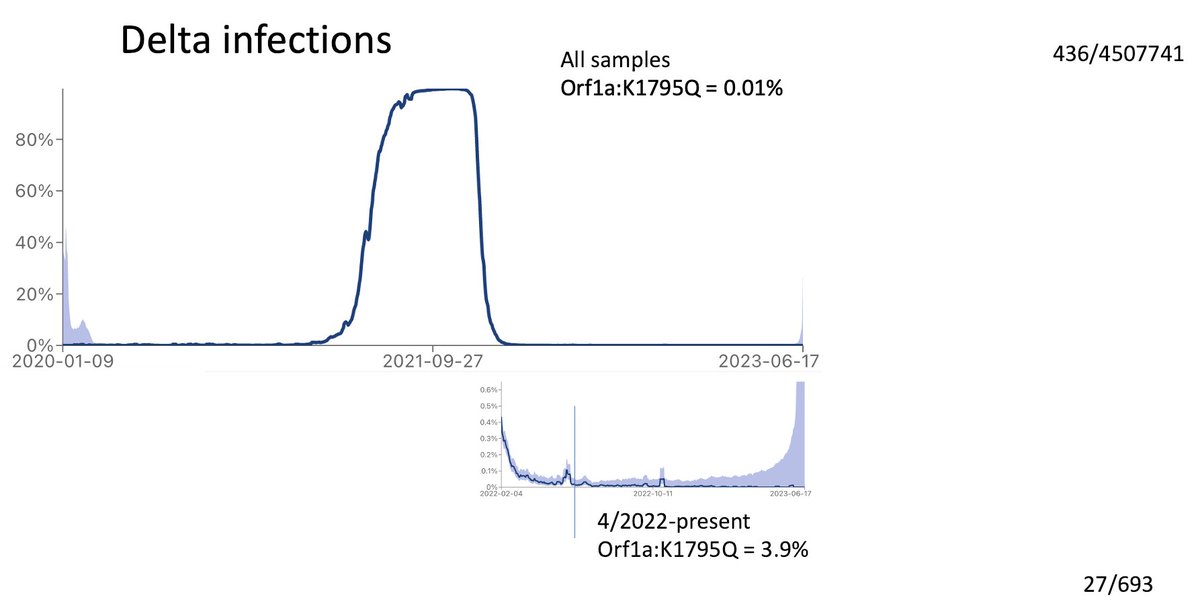
How frequent is K1795 in chronic Delta infections.
Delta mostly disappeared in Jan, 2022, so by April, the Delta infections were pretty much all chronic.
K1795Q was in less than 0.01% of all Delta sequences, but was present in almost 4% of the sequences after April, 2022.
3/
Delta mostly disappeared in Jan, 2022, so by April, the Delta infections were pretty much all chronic.
K1795Q was in less than 0.01% of all Delta sequences, but was present in almost 4% of the sequences after April, 2022.
3/
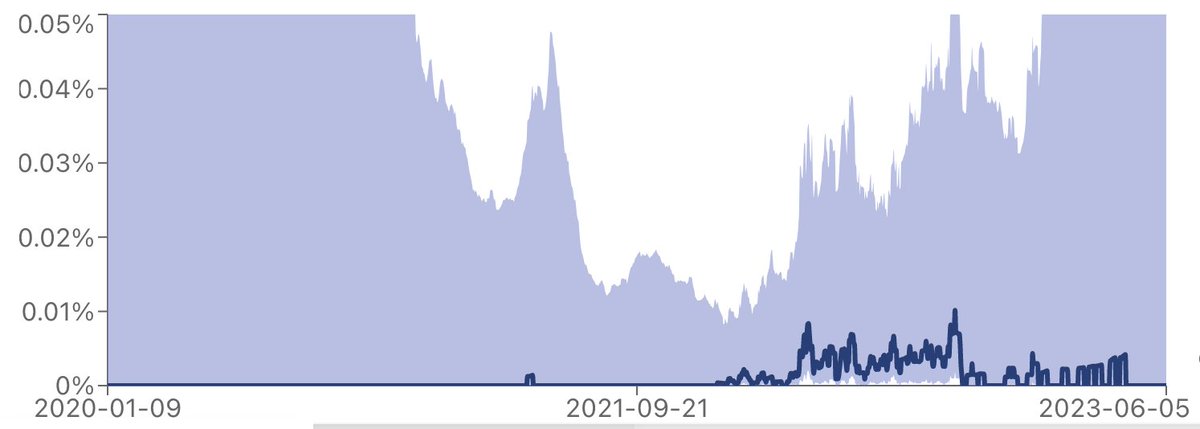
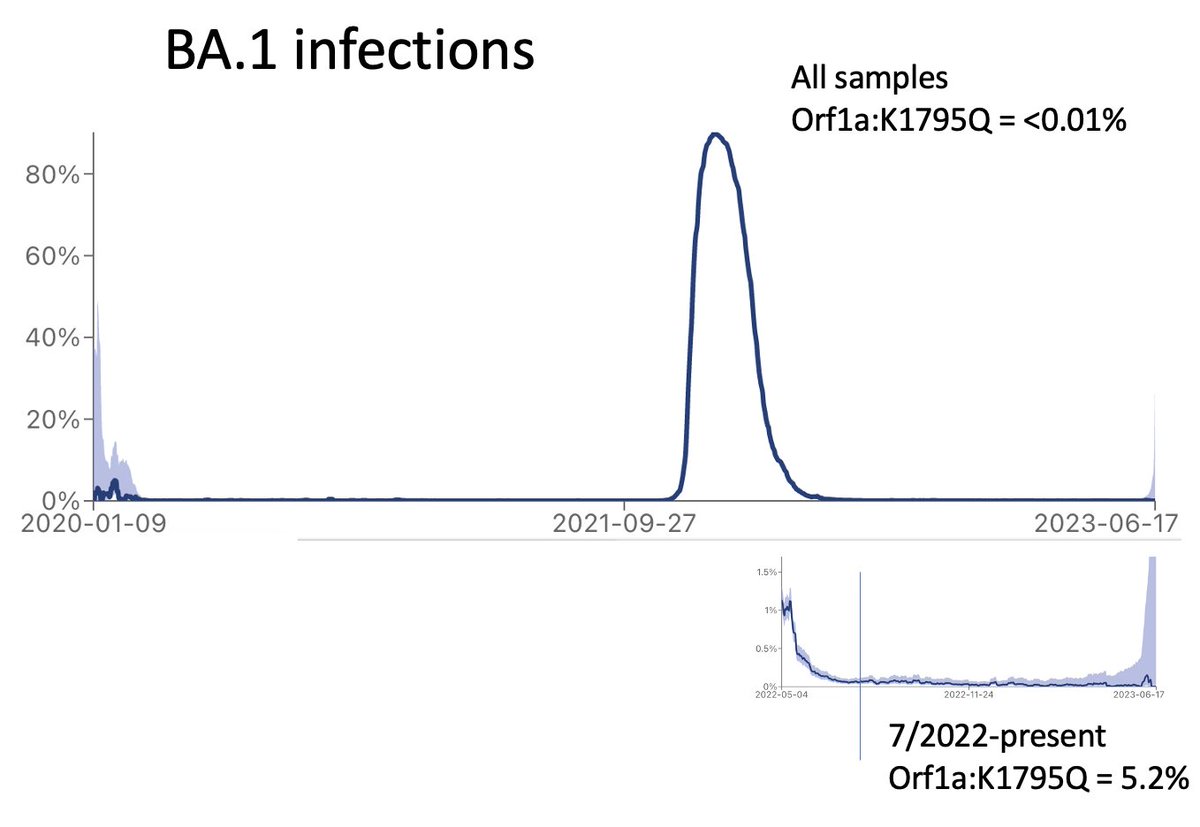
What about BA.1? BA.1 was dominant from Dec, 2021-March, 2022.
By July the infections were pretty much gone other than chronic infections.
The frequency of K1795Q in BA.1 went from <0.01% overall, to over 5% from samples collected after July 2022.
4/
By July the infections were pretty much gone other than chronic infections.
The frequency of K1795Q in BA.1 went from <0.01% overall, to over 5% from samples collected after July 2022.
4/
Caveat, some of this data is imperfect. At least some of the samples just had the wrong date entered, and at least some of the chronic cases represent patients that were sampled multiple times.
It is not trivial trying to sort this out.
5/
It is not trivial trying to sort this out.
5/
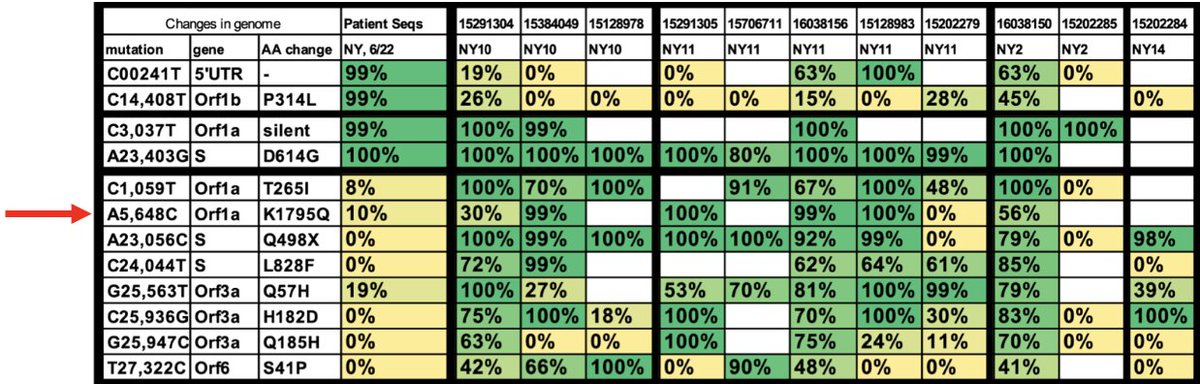
I also asked @LongDesertTrain (who tracks all chronic sequences) to give me a list of his 50 clearest Omicron-derived chronic infections based on their sequence divergence.
Even among these extreme chronic infections (more likely to have it), K1795Q was still only in 18%.
6/
Even among these extreme chronic infections (more likely to have it), K1795Q was still only in 18%.
6/
Taken together, I would say that probably about 4-10% of chronic infection sequences contain K1795Q, and K1795Q rarely appears in non-chronic infections.
7/
7/
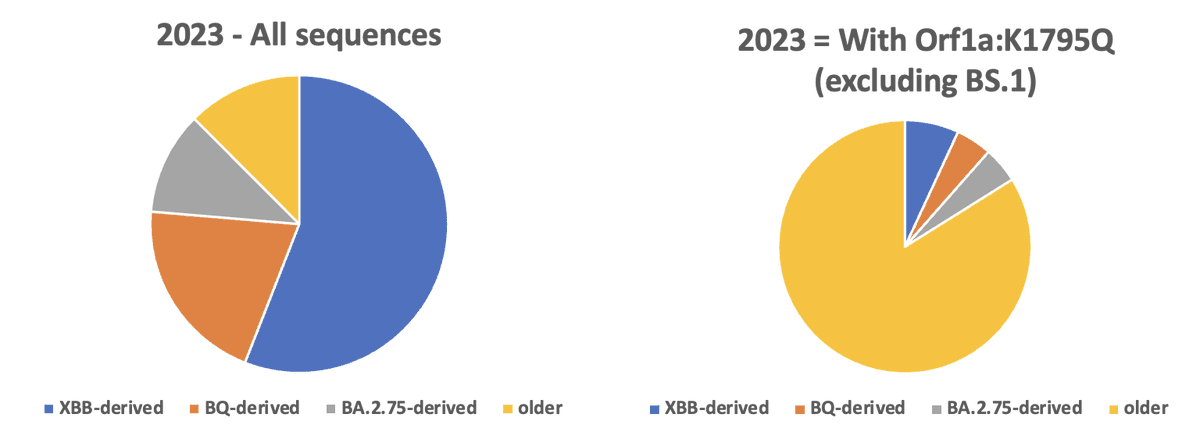
Here is another way to look at it. If you consider all SC2 sequences deposited in 2023, only 12% was an ‘older’ lineage (not XBB-, BQ-, or BA.2,75-derived).
However, among sequences from 2023 containing K1795Q (excluding BS.1), about 84% were ‘older’.
8/
However, among sequences from 2023 containing K1795Q (excluding BS.1), about 84% were ‘older’.
8/
So how common are chronics?
In the last year there have been 374 sequences (excluding BS.1) containing K1795Q. If we assume that this represents 4-10% of all of the chronic sequences, there would have been around 3,740-9,350 chronic sequences, or 0.1%-0.3% of all sequences.
9/
In the last year there have been 374 sequences (excluding BS.1) containing K1795Q. If we assume that this represents 4-10% of all of the chronic sequences, there would have been around 3,740-9,350 chronic sequences, or 0.1%-0.3% of all sequences.
9/
I know that these calculations aren’t perfect, but I think they get you in the ballpark.
10/
10/
The bigger question for me is whether chronic infections are more or less likely to be tested and sequenced. Could be skewed either way. However, if some people have chronic infections outside of the nasal tract (and I suspect they do), then I know that these are unsampled.
11/
11/
No matter how you slice it, there are still a lot of chronic infections that people are still dealing with. It would be great if we could do more to help these patients.
12/
12/
• • •
Missing some Tweet in this thread? You can try to
force a refresh