🧀🧀
Pharma and government activist die-hards who were desperate to claim the COVID vaccines reduced infection rates - when they ended up increasing infection rates - often flail and refer to the footnotes added to the @UKHSA by @SarahCaul_ONS's team.
This thread debunks them https://t.co/Q24Lxs38fO https://t.co/nt3mFqC0Vntwitter.com/i/web/status/1…

Pharma and government activist die-hards who were desperate to claim the COVID vaccines reduced infection rates - when they ended up increasing infection rates - often flail and refer to the footnotes added to the @UKHSA by @SarahCaul_ONS's team.
This thread debunks them https://t.co/Q24Lxs38fO https://t.co/nt3mFqC0Vntwitter.com/i/web/status/1…
https://twitter.com/Jikkyleaks/status/1673863279058509828

This is the actual footnote in the A4 landscape page 45 of the report.
Remember that this was the last UKHSA report to provide infection rates by vaccine status per 100,000 (per capita)
@SarahCaul_ONS got orders to stop reporting these rates because they were embarrassing.
Remember that this was the last UKHSA report to provide infection rates by vaccine status per 100,000 (per capita)
@SarahCaul_ONS got orders to stop reporting these rates because they were embarrassing.

For readability I have copy/pasted this to portrait and increased the font size, but it's still a lot of words.
351 to be precise.
Let's go through it to see how ridiculous it is.
351 to be precise.
Let's go through it to see how ridiculous it is.

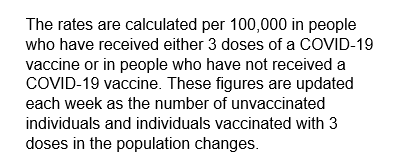
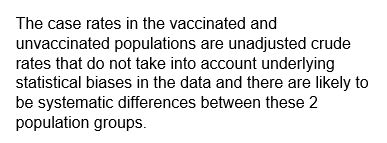
The second paragraph explains that these are case rates *per 100,000* people in each group.
Exactly the data required to calculate effectiveness of a vaccine.
Perfect.
Exactly the data required to calculate effectiveness of a vaccine.
Perfect.
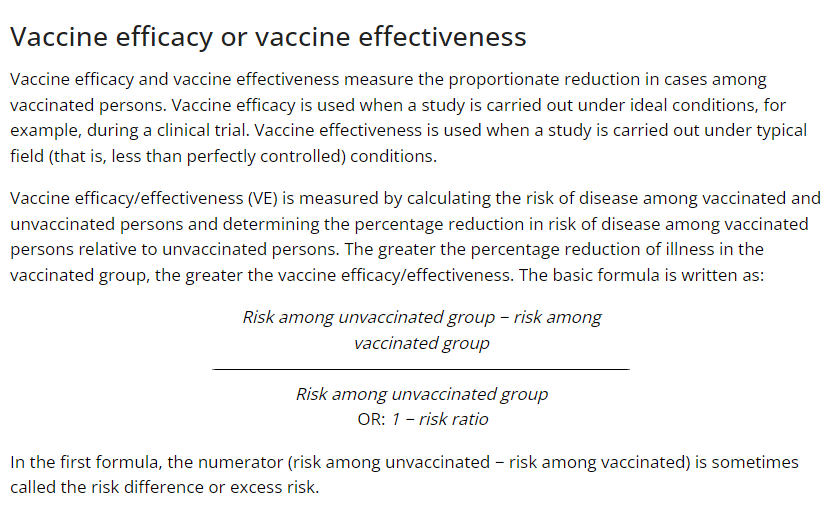
For reference, this is the official calculation of vaccine effectiveness (which has been used in the coloured table at the start of this thread).
Please do the calculations yourself if you don't agree.
https://t.co/9hwCdp3SwRcdc.gov/csels/dsepd/ss…
Please do the calculations yourself if you don't agree.
https://t.co/9hwCdp3SwRcdc.gov/csels/dsepd/ss…
Now we get to the excuses. This is a doozy.
They are literally telling you to ignore decades of epidemiology, because it doesn't give them the answer they were programmed for.
@vnafilyan who is the main player at the UKHSA should be permanently embarrassed by this statement
They are literally telling you to ignore decades of epidemiology, because it doesn't give them the answer they were programmed for.
@vnafilyan who is the main player at the UKHSA should be permanently embarrassed by this statement
What they want you to accept is that you should ignore the ACTUAL data and accept an ESTIMATE which is not even based on their own data.
No, this is actually what they say.
No, this is actually what they say.
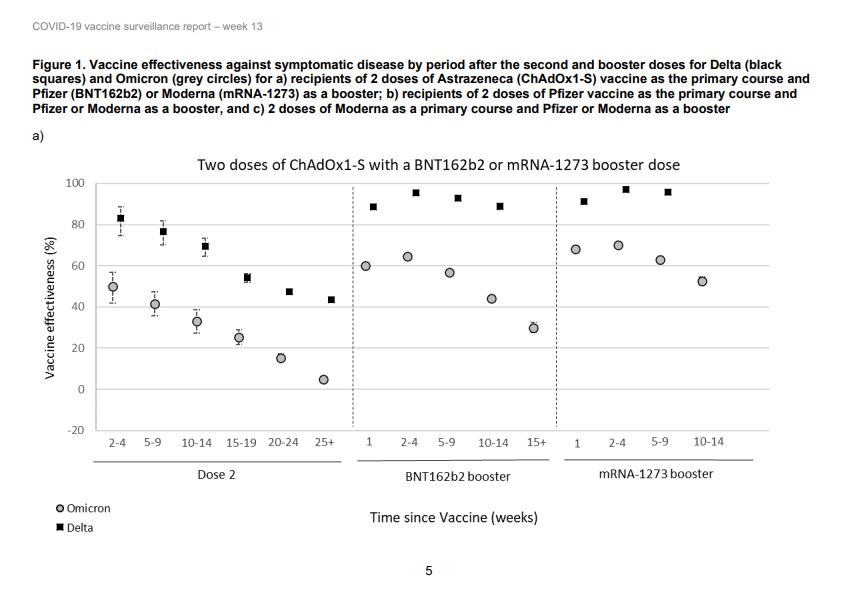
They did it to excuse the use of other data sets (biased retrospective studies which used temporal miscategorisation to mimic efficacy) instead of using the actual data they had.
Then published the laundered data at the start of the document (p5), and changed the comparator
Then published the laundered data at the start of the document (p5), and changed the comparator
Note the rates that were provided were the "unadjusted" rates per 100,000. So that is not accounting for any differences in the type of people that were vaccinated vs unvaccinated.
It doesn't matter. The biggest confounder was age, which was separated out...
It doesn't matter. The biggest confounder was age, which was separated out...
So what other confounders could they be thinking of?
They shot themselves in the foot even here, because they were basically admitting that people who avoided the vaccine were either smarter or healthier than those who didn't.
They shot themselves in the foot even here, because they were basically admitting that people who avoided the vaccine were either smarter or healthier than those who didn't.
And so they had to flail a bit more, and this gets more entertaining.
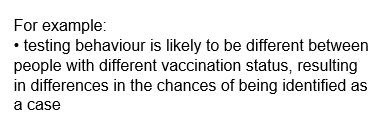
Vaccinated were testing more? Really? On which planet was that? People tested less when they were vaccinated because they thought they were safe.
Vaccinated were testing more? Really? On which planet was that? People tested less when they were vaccinated because they thought they were safe.
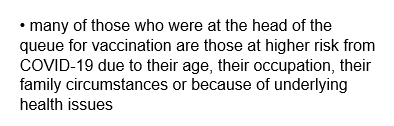
Age? You already broke it down by age so you can discount that.
Occupation? That basically means healthcare workers - so you're saying that vaccinated healthcare workers had a higher risk of infection than unvaccinated non-HCWs.
Great work NHS.
Occupation? That basically means healthcare workers - so you're saying that vaccinated healthcare workers had a higher risk of infection than unvaccinated non-HCWs.
Great work NHS.
I mean, did they come up with this at a Tory party get together?
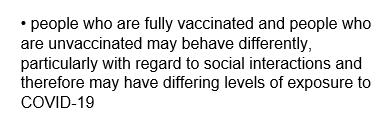
"The vaccinated get more COVID because they go out more"?
Better avoid those people then.
The flailing is off the scale.
"The vaccinated get more COVID because they go out more"?
Better avoid those people then.
The flailing is off the scale.

And this one is a corker.
Literally admitting that natural immunity provides protection from *infection*.
Whoever decided to add this one should have been given a bonus.
Literally admitting that natural immunity provides protection from *infection*.
Whoever decided to add this one should have been given a bonus.
Finally the biggest embarrassment of all "we use NIMS so we don't really know what the real rates are, but take the vaccine anyway"
@ClareCraigPath and @profnfenton have done loads of work on the failure of these datasets.
@ClareCraigPath and @profnfenton have done loads of work on the failure of these datasets.
Yes those are the excuses that the #Vaccinati came up with to tell you not to do your own calculations using their data.
It's literally a rerun of this classic from 2017...
(Clipped from ) https://t.co/O4ShCUGNlc
It's literally a rerun of this classic from 2017...
(Clipped from ) https://t.co/O4ShCUGNlc
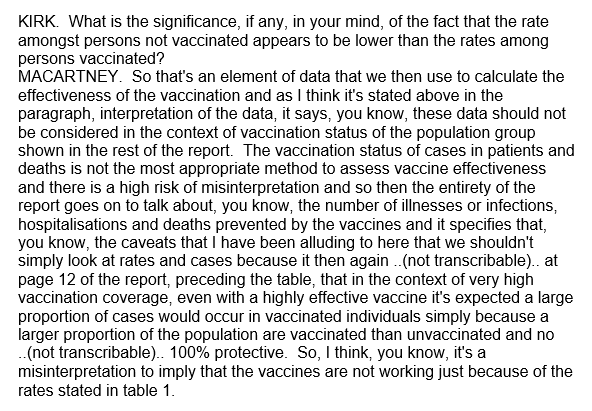
If anyone tells you (like the $65m vaccinologist, Kristine Macartney, in Kassam vs Hazzard - transcript below) that you can't use the official UKHSA data to show that the vaccine *increases* infection rates.
Send them this thread. Then mock them relentlessly.
@TonyNikolic10
Send them this thread. Then mock them relentlessly.
@TonyNikolic10
*2016
And don't forget the broken flailing gif when you do!
https://t.co/CNctVK3v9k
https://t.co/CNctVK3v9k
https://twitter.com/Jikkyleaks/status/1675005467914043397?s=20
Proof that the @ONS @UKHSA got orders to push this propaganda... from Ed Goebbels-Humpherson "Director of Regulation"
If the data doesn't support your drug, perhaps your drug doesn't actually work.
https://t.co/bNJwnRjlQwarchive.is/AqHbB
If the data doesn't support your drug, perhaps your drug doesn't actually work.
https://t.co/bNJwnRjlQwarchive.is/AqHbB
https://twitter.com/HopkinsonJason/status/1675015113273667584?s=20
@ONS @UKHSA

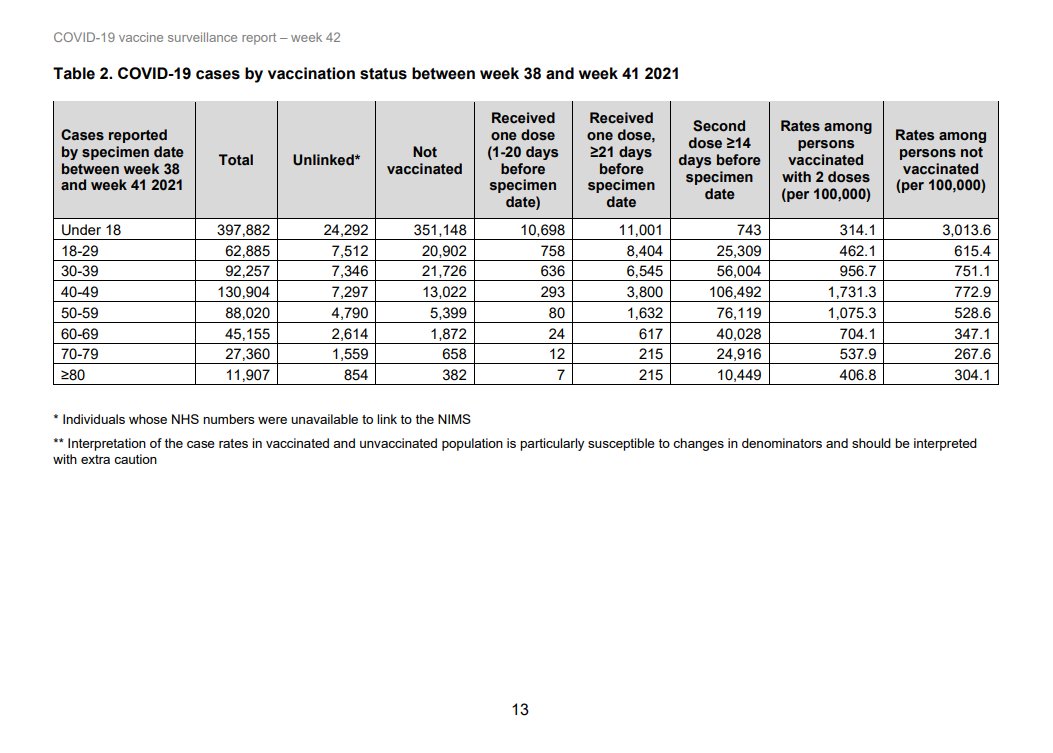
Good point. Here is a report from a few weeks earlier. Note the rates by vaccine status are in Table 2 (instead of buried in Table 14) and on page 13 (not 45)
The case rate was low for a few weeks after vaccination, then after that time exceeded the unvaccinated in all age… https://t.co/mqta9IwZUPtwitter.com/i/web/status/1…
The case rate was low for a few weeks after vaccination, then after that time exceeded the unvaccinated in all age… https://t.co/mqta9IwZUPtwitter.com/i/web/status/1…
• • •
Missing some Tweet in this thread? You can try to
force a refresh