THEY ARE USING THIS TO KILL US
THE DISTURBING TRUTH BEHIND “ANTIDEPRESSANTS” (SSRIs)
LONG THREAD https://t.co/ei75OufYlRtwitter.com/i/web/status/1…

THE DISTURBING TRUTH BEHIND “ANTIDEPRESSANTS” (SSRIs)
LONG THREAD https://t.co/ei75OufYlRtwitter.com/i/web/status/1…


We released our video on the topic about 2 years ago, which dives deep into the story of serotonin.
The monoamine hypothesis of depression has and continues to guide the medical establishment and collective consciousness on depression.
This theory states that a depletion of monoamine neurotransmitters, dopamine, norepinephrine and serotonin, leads to “depression.”
This theory states that a depletion of monoamine neurotransmitters, dopamine, norepinephrine and serotonin, leads to “depression.”
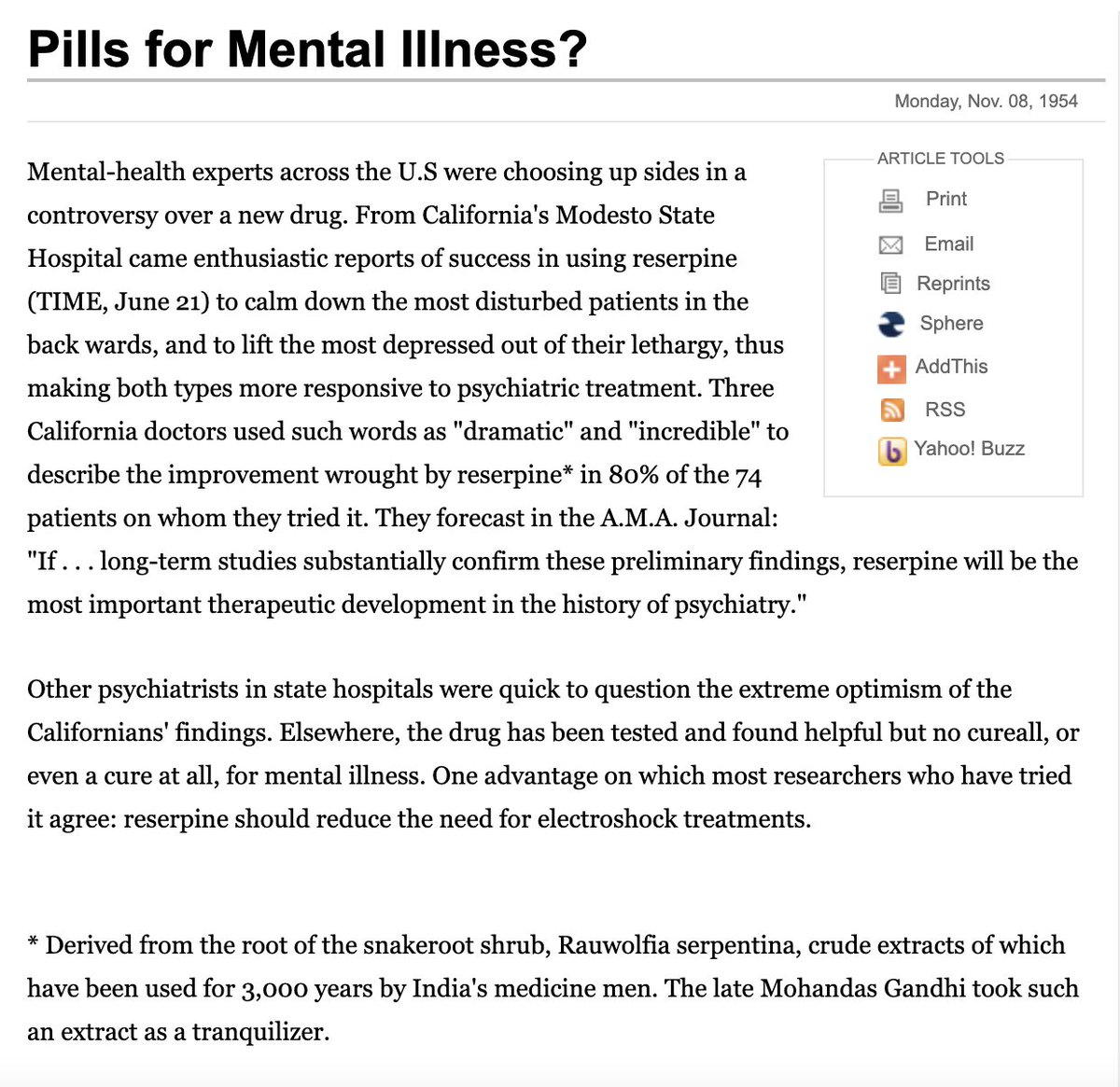
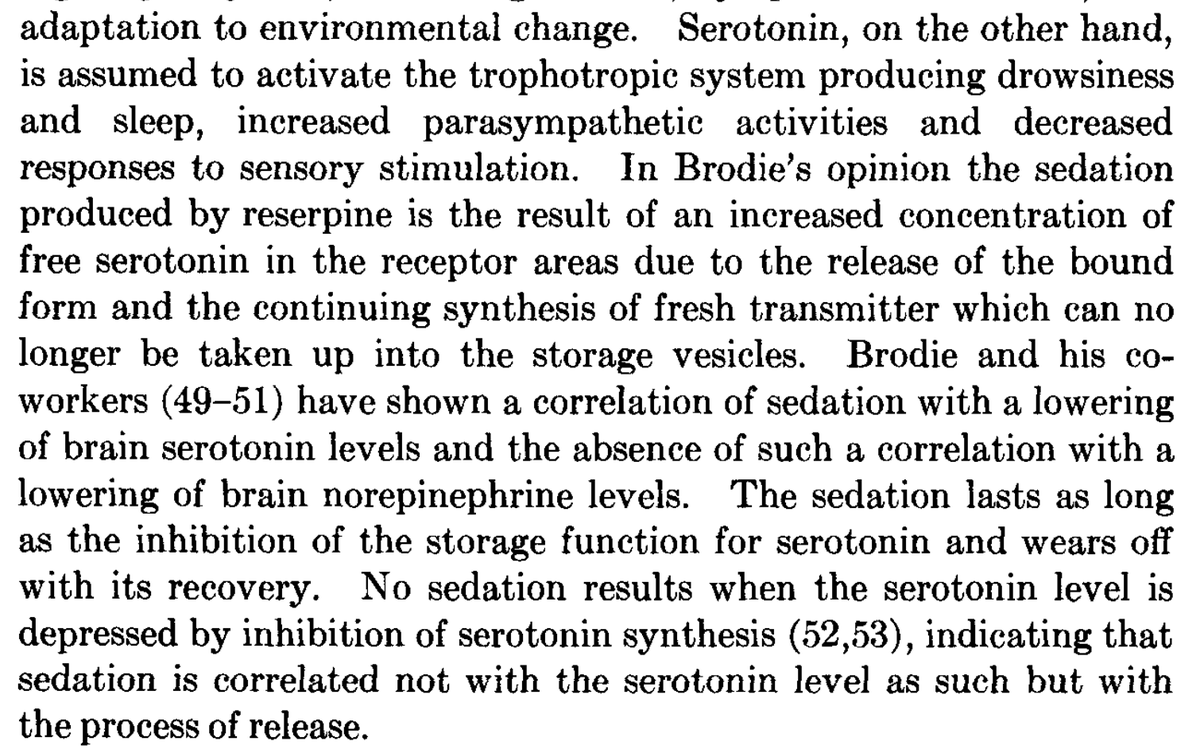
Reserpine, a drug that had been used for centuries by Indians.
Even Ghandi used it.
Reserpine works by inhibiting the release of all monoamines.
Despite showing benefit in humans, the narrative became that it induced depression in animals due to its sedative properties.
Even Ghandi used it.
Reserpine works by inhibiting the release of all monoamines.
Despite showing benefit in humans, the narrative became that it induced depression in animals due to its sedative properties.
This "theory" lead to the creation of various drugs that are still in wide use today.
Monoamine oxidase inhibitors prevent breakdown of these compounds, while tricyclics act as dopamine, serotonin and norepinephrine reuptake inhibitors, also increasing their amount.
Monoamine oxidase inhibitors prevent breakdown of these compounds, while tricyclics act as dopamine, serotonin and norepinephrine reuptake inhibitors, also increasing their amount.
However, since then the reserpine-induced depression model has been characterized as a myth by various researchers.
Recent reviews have stated that reserpine, at best does not consistently induce depression, and in many cases can treat it! ncbi.nlm.nih.gov/pmc/articles/P…
Recent reviews have stated that reserpine, at best does not consistently induce depression, and in many cases can treat it! ncbi.nlm.nih.gov/pmc/articles/P…
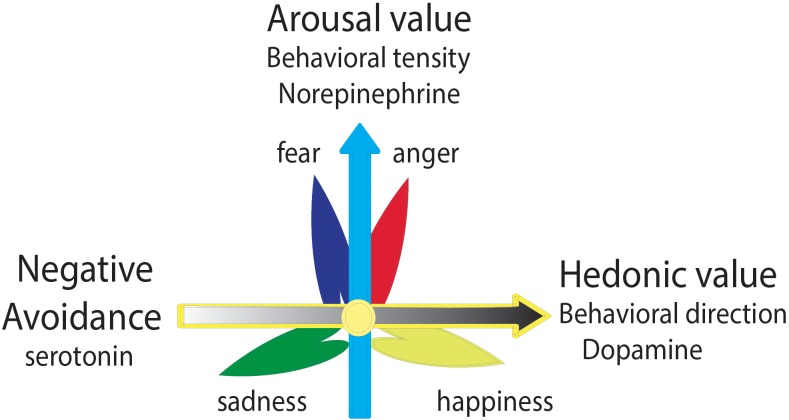
This should come as no surprise given that these 3 neurotransmitters all have remarkably different effects on mood and perspective.

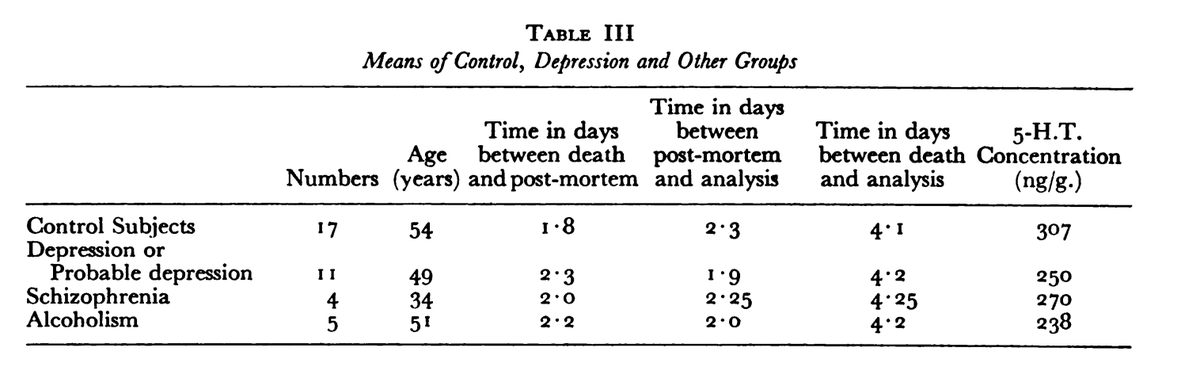
Some small studies suggested a link between lower serotonin levels in certain brain regions post mortem, further driving the hypothesis.
The authors cautioned that these findings were preliminary and did not do much but allow them to test more hypotheses.
The authors cautioned that these findings were preliminary and did not do much but allow them to test more hypotheses.
Pharma giant Lilly went to work quickly on developing drugs that selectively increased serotonin.
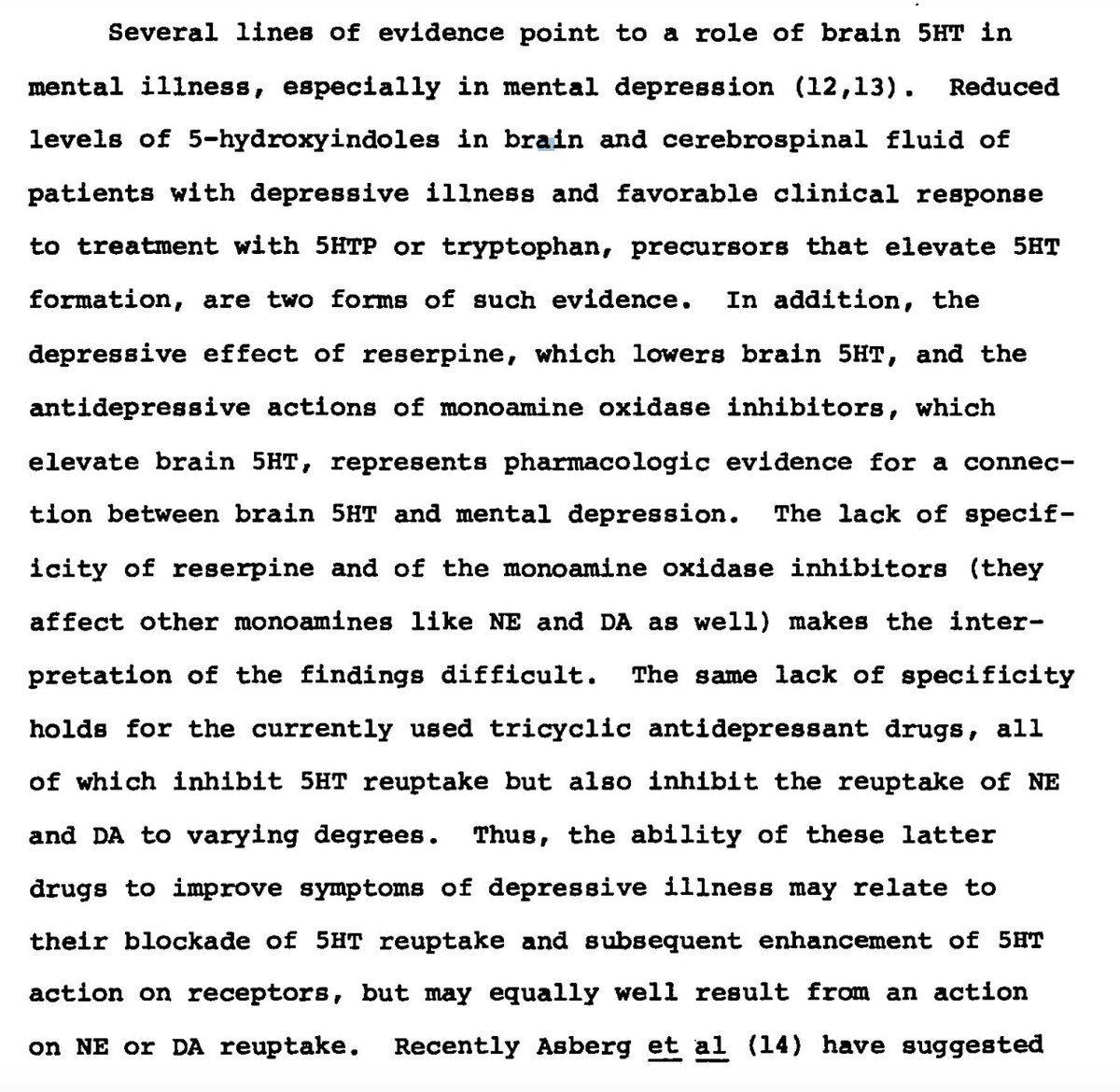
In their original manuscript, they claim that there is multiple lines of evidence suggesting serotonin is low in depression,
but their references don’t remotely support this.
In their original manuscript, they claim that there is multiple lines of evidence suggesting serotonin is low in depression,
but their references don’t remotely support this.
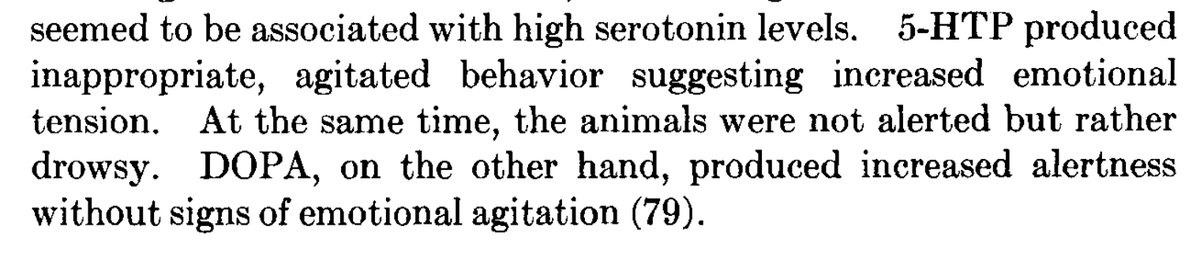
In fact, it supported the exact opposite: administering serotonin precursors caused sedation, numbness, convulsions, tremors and agitation.
Dopamine precursors produced alertness with none of these “side effects.”
Dopamine precursors produced alertness with none of these “side effects.”

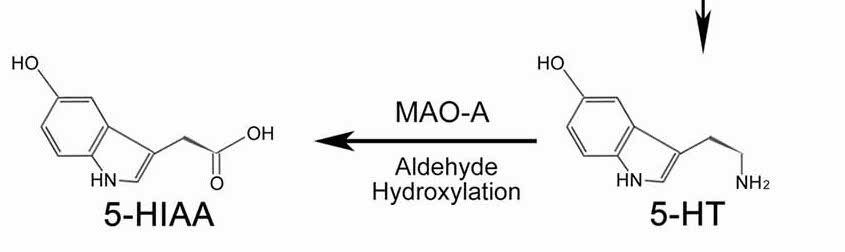
They also note that 5HIAA cerebrospinal fluid concentrations, which is the “deactivated” version of serotonin, were decreased in certain mental illness.
They went ahead and assumed that this was because they had less serotonin generally, not because they had less turnover!
They went ahead and assumed that this was because they had less serotonin generally, not because they had less turnover!

So it becomes clear rather quickly that tTeuptake Inhibitors (SSRIs) were not only completely unfounded, but were likely intentional given what we’ve discussed previously: that serotonin makes people easy to manipulate:
https://twitter.com/Outdoctrination/status/1676983469694672896
Documentation from LIlly in 1984 showed that severe agitation leading to suicide occurred in over 1% of patients, a figure large enough that it was required to be disclosed to regulatory agencies.
Of course, Lilly excluded this when seeking approval.
old.narpa.org/prozac.revisit…
Of course, Lilly excluded this when seeking approval.
old.narpa.org/prozac.revisit…
Lilly first tried to get Prozac approved in Germany, with their drug regulatory agency saying in a fax back to Lilly that “we think this preparation totally unsuitable for the treatment of depression.”
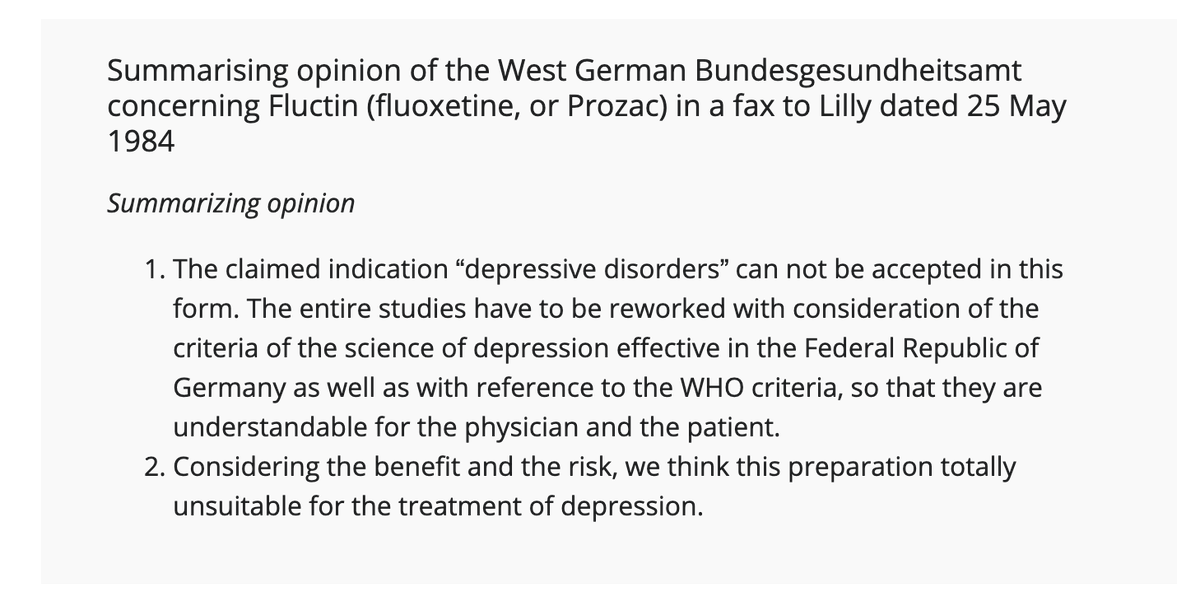
This hilarious reaction was driven by the fact that after reviewing Prozac’s trial data, it was painfully obvious that many patients would take the drug and go on to commit suicide.
“it refused to approve the antidepressant based on Lilly's studies showing that previously nonsuicidal patients who took the drug had a 5 fold higher rate of suicides and suicide attempts than those on older antidepressants, and a 3 fold higher rate than those taking placebos.”
Despite this clear evidence that Prozac was outright dangerous and made people kill themselves, the FDA approved Prozac in 1987, and it quickly became one of the hottest drugs on the market.
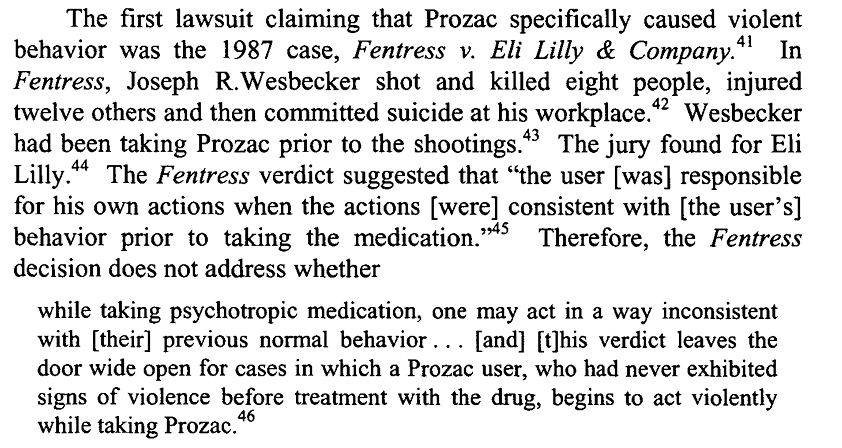
In 1987, the first lawsuit involving Prozac and violent tendencies was initiated.
A man who was taking Prozac shot and killed eight people, injured twelve others and then committed suicide at his workplace.
The verdict was that it had nothing to do with Prozac.
A man who was taking Prozac shot and killed eight people, injured twelve others and then committed suicide at his workplace.
The verdict was that it had nothing to do with Prozac.
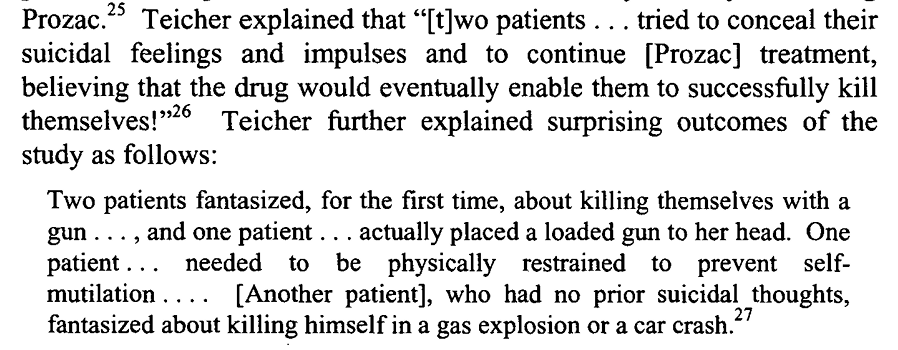
In 1990, shortly after Prozac’s approval, Harvard psychiatrist Martin H. Teicher reported that SSRIs could cause suicidal or homicidal tendencies. He described cases in disturbing, gory detail.
It was clear that these individuals had their reality distorted.
It was clear that these individuals had their reality distorted.
Lilly scientists were pressured by executives to alter records on doctor experiences with Prozac: changing mentions of “suicide attempts” to "overdose" and suicidal thoughts to "depression."
Once again we have clear indication that they knew exactly what they were doing
Once again we have clear indication that they knew exactly what they were doing
One LIlly employee stated:
“I do not think I could explain to [anyone] why we would do this especially on the sensitive issue of suicide and suicide ideation. At least not with the explanations that have been given to our staff so far.”
“I do not think I could explain to [anyone] why we would do this especially on the sensitive issue of suicide and suicide ideation. At least not with the explanations that have been given to our staff so far.”
Lilly also withheld data demonstrating that “Prozac may produce nervousness, anxiety, agitation, or insomnia in 19% of users and sedation in 13% of users”
The FDA became aware of this deliberate manipulation. The chief FDA epidemiologist stated:
“Because of apparent large-scale underreporting, the firm's analysis cannot be considered as proving that fluoxetine and violent behavior are unrelated."
“Because of apparent large-scale underreporting, the firm's analysis cannot be considered as proving that fluoxetine and violent behavior are unrelated."
Despite massive evidence to the contrary, in 1991 the FDA concluded that there was no evidence for a causal link between Prozac and violence. Shocking.

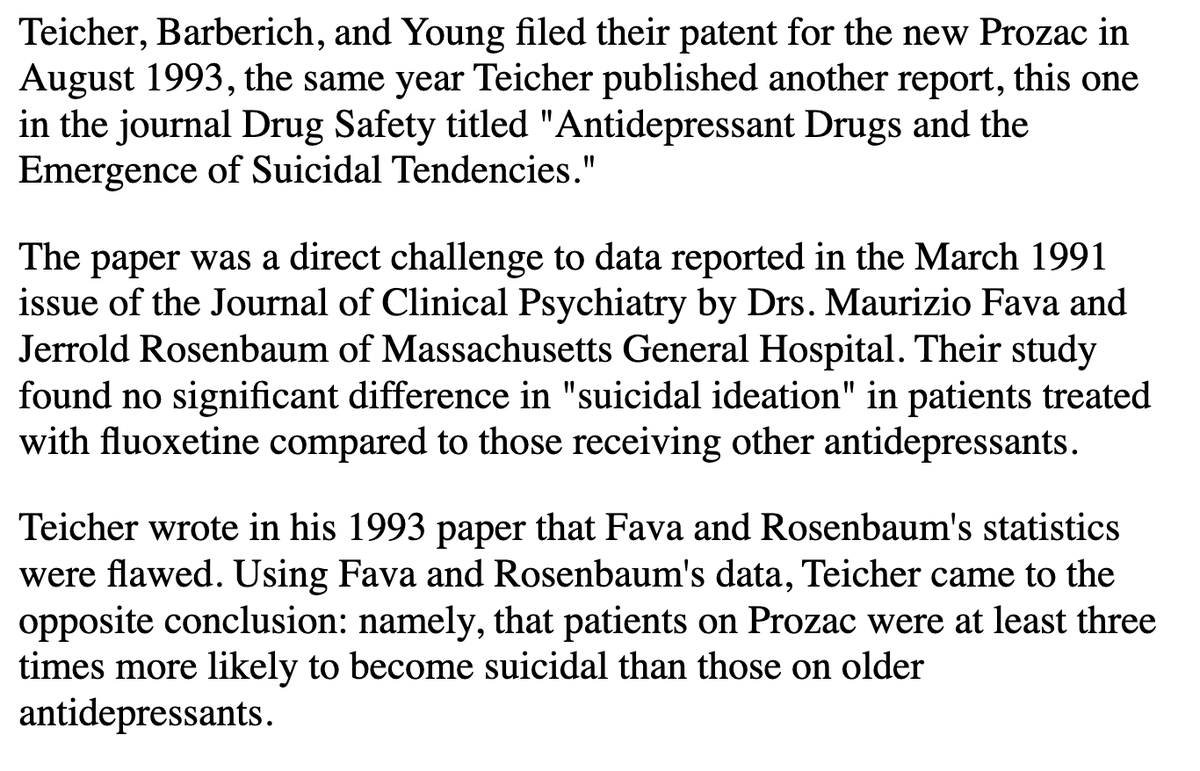
Lilly also had hired guns to dismiss these notions. Researchers they had on staff churned out questionable statistical analysis that “disproved” Teicher’s concerns, but Teicher pointed out the flaws in their work.
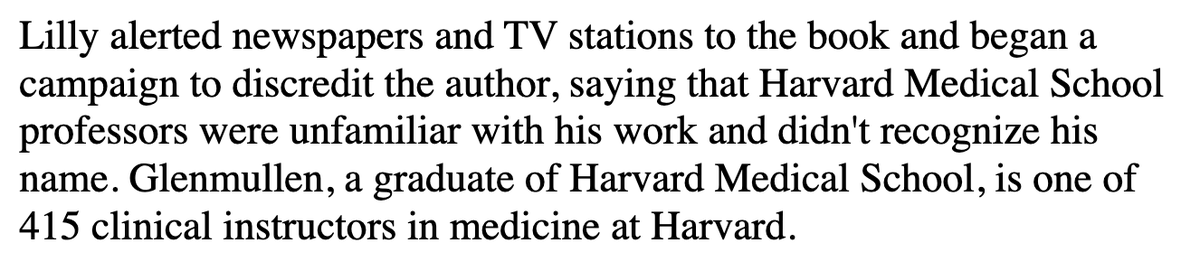
Lilly later initiated a media smear campaign against another Harvard doctor published the book Prozac Backlash, detailing Lilly’s malpractice and tendency to hide or downplay harms of their drug. https://t.co/7h9PTqCGRItwitter.com/i/web/status/1…
Things came to a climax at the Tobin v. SmithKline trial, where an individual shot and killed his wife, daughter, granddaughter, and himself after just two doses of Praxil, another SSRI drug. Finally, Pharma was held (somewhat) accountable, as the jury found for the plaintiff.
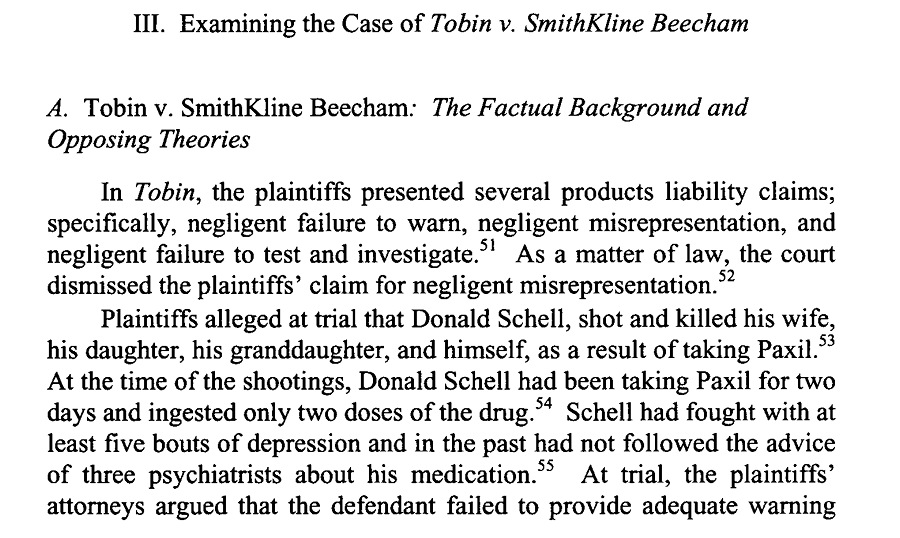
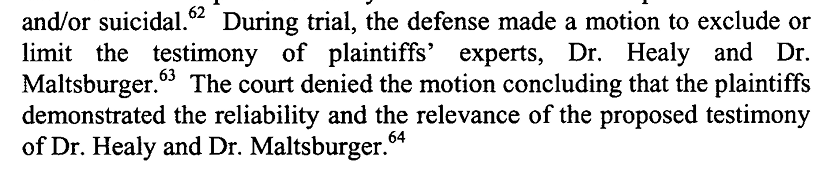
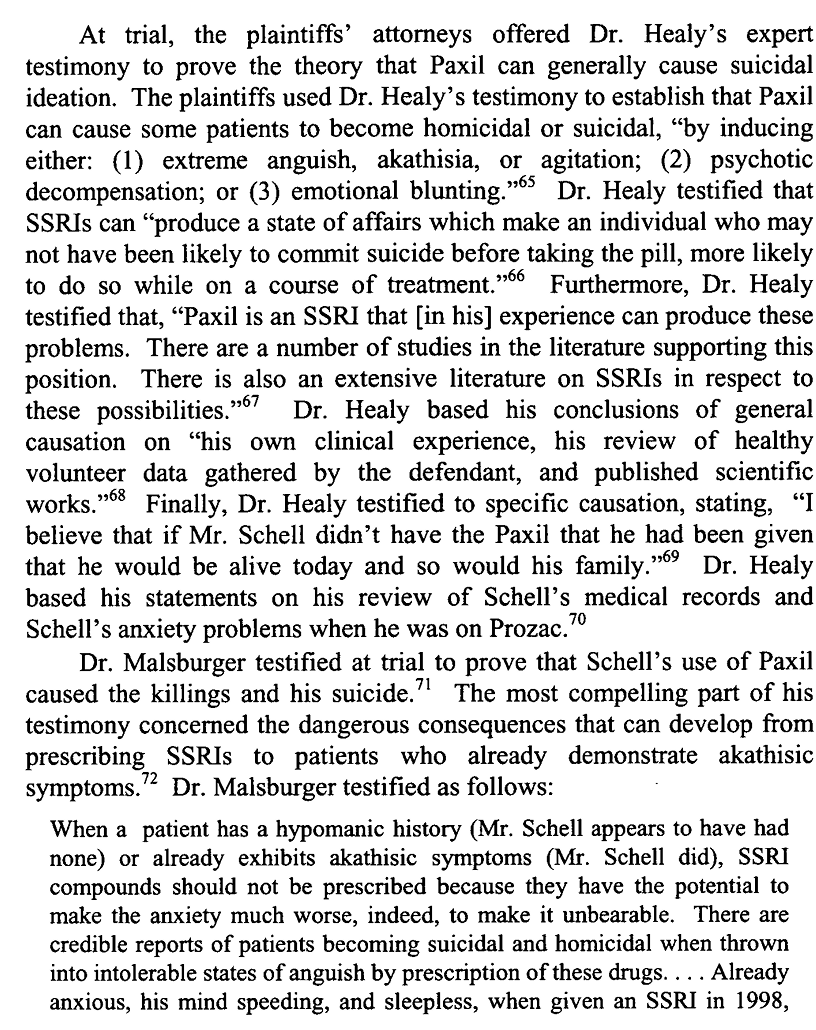
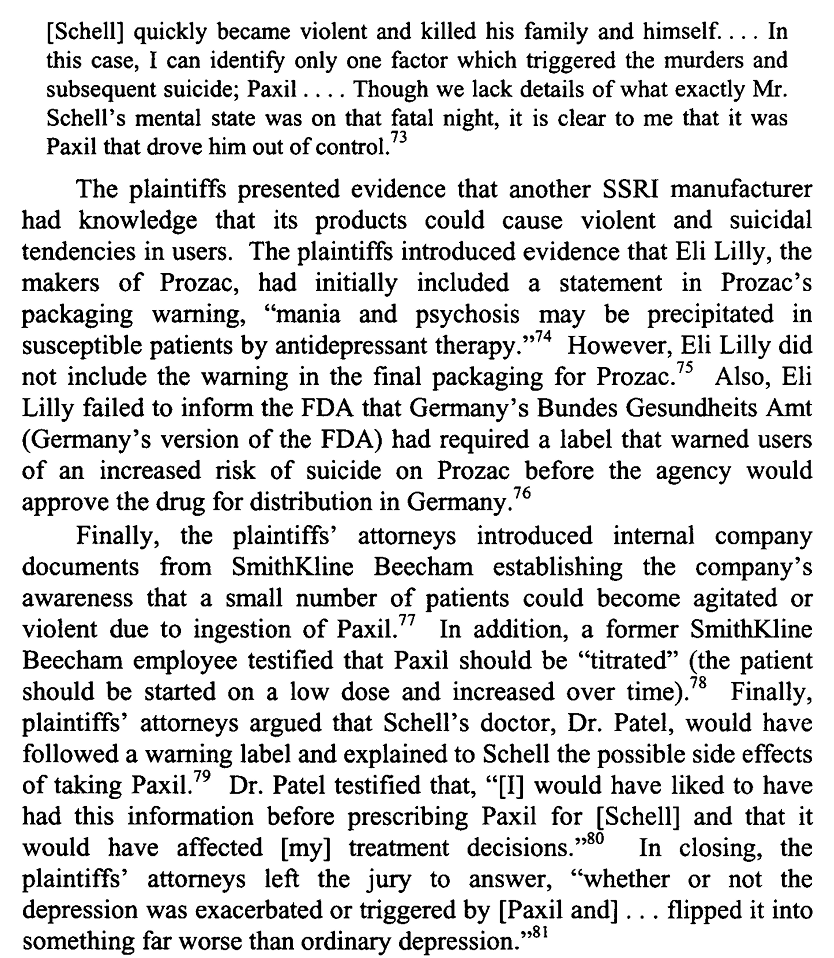
Doctors testified, saying that there was already a extensive existing literature on how SSRIs could cause suicidal or homicidal tendencies. They presented substantial evidence that both Lilly and SmithKline were well aware of this. twitter.com/i/web/status/1…
Several other trials were held about similar issues: people starting to take SSRIs and then killing others and/or themselves.
By this point it didn’t matter. Prozac was a top 5 selling drug and was raking in billions. Paying off a few million to some families was well worth it.
By this point it didn’t matter. Prozac was a top 5 selling drug and was raking in billions. Paying off a few million to some families was well worth it.
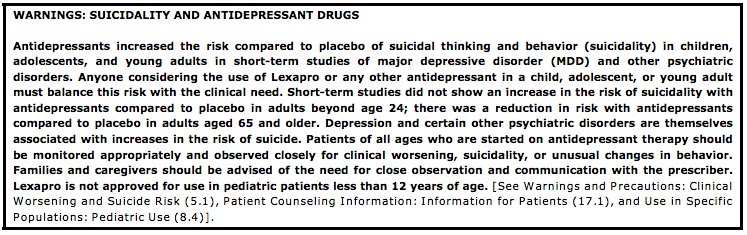
In 2004, the FDA finally issued a blackbox warning on these medications of a “link” between taking them and violence and/or suicide and worsened depression. Zoloft, Lexapro, Prozac and Celexa continue to make billions, being handed out to tens of millions of Americans yearly.
Oh yeah, but you know, it was just an accident.
They didn’t know any better. More studies are needed.
Give me a f*cking break.
This is pure evil twitter.com/i/web/status/1…
They didn’t know any better. More studies are needed.
Give me a f*cking break.
This is pure evil twitter.com/i/web/status/1…
Thanks for reading through this thread, we will have plenty of more content on this issue soon. Toss us a RT if you enjoyed, and be sure to check out all of our content, consultation options and supplements over at lnk.bio/analyze.and.op…
• • •
Missing some Tweet in this thread? You can try to
force a refresh