Exercises for Medial Tibial Stress Syndrome (AKA Shin ‘Splints’) A thread 🧵
👉🏻 Inspired by @tomgoom
👉🏻 Inspired by @tomgoom

1) Way too often in rehab, people talk about strengthening x, y and z, improving movement control etc. but never what it really means. This thread covers an exercise program used for someone with MTSS and the reasoning behind it.
2) The patient is a young male middle-distance runner who shows a mild weakness in the Soleus, Glute Med and posterior chain. Our aims are as follows: improving local load capacity of the calves and kinetic chain & including weight-bearing exercises to improve bone load capacity.

3) Gluteal muscles are vital in absorbing load during the stance phase of running. Step ups will activate Glute Max and Med and will provide a proprioceptive challenge. Hip hitches aka pelvic drops and side lying leg lifts will also target the Glute Med very nicely.
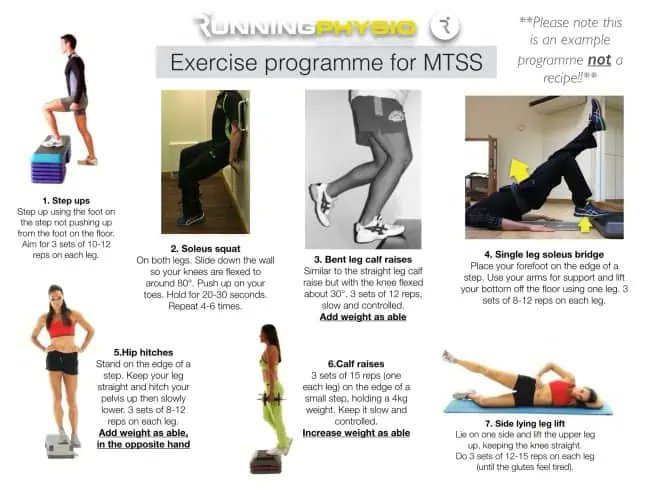
4) The Soleus is thought to be particularly important in MTSS as it helps reduce the bending force that the tibia experiences during impact. Bent leg calf raises & soleus squats are great exercises. The latter will also target the quads, which helps absorb load during running.

5) A single leg soleus bridge will lengthen the lever to challenge the posterior chain and work the soleus. Do note that the soleus load is rather low, but it will challenge the Glute Max and hamstrings which are most active during swing phase and contribute to the loading phase.

6) Classic straight leg calf raises will strengthen the gastroc & soleus and reduce bone load. Forefoot strikers experience a particularly higher load in the calf complex so make sure they have adequate strength to manage this load.

7) These exercises are not a recipe for MTSS but rather a snapshot of one patient’s exercises and why they’re valuable. It’s important to review, adapt and progress the rehab at each session and make it part of a comprehensive management program.
That’s a wrap on this thread, thanks for making it ‘til the end!
Make sure to read Tom Goom’s full blog if you want to know more about this topic.
You can read the full blog using the following link:
physio-network.com/blog/exercises…
Make sure to read Tom Goom’s full blog if you want to know more about this topic.
You can read the full blog using the following link:
physio-network.com/blog/exercises…
• • •
Missing some Tweet in this thread? You can try to
force a refresh