I recently gave a COPD boot camp lecture and wanted to share some of the high points. 🫁
#tipsfornewdoctors
#tipsfornewdoctors
Much of this content comes from the 2023 GOLD report + the 2005 and 2022 PFT interpretation papers (these are great resources to keep handy). 

In general, COPD = respiratory symptoms + obstruction + h/o exposure. To learn about COPD, you first have to learn about obstruction.
This is a flow volume loop. Yellow is the inspiratory limb (patient breathing in), and red is the expiratory limb (patient blasting out).
This is a flow volume loop. Yellow is the inspiratory limb (patient breathing in), and red is the expiratory limb (patient blasting out).

This is an obstructed loop (orange) vs a normal loop (blue). The classic appearance of obstruction is scooping of the expiratory limb, indicating impaired expiratory flow (due to narrowed airways).

Because inflammation, mucus, and smooth muscle hypertrophy have narrowed the airways, it takes a longer time for these patients to exhale. This means less air forced out in 1 second (the FEV1). The total amount they can exhale is preserved, which is why the FEV1/FVC ratio drops.

When assessing the FEV1/FVC ratio the most recent guidelines discourage use of a fixed 0.7 cutoff due to systematic misinterpretation. I use the LLN (no z-scores on our PFTs yet).
See Mannino (Thorax 2007) for LLN vs fixed cutoff graph.
See Mannino (Thorax 2007) for LLN vs fixed cutoff graph.



Granted, the closer you are to that LLN (5th percentile), the more uncertain you have to be about whether or not actual obstruction is present and the more you have to rely on your clinical assessment of the patient.
(Haynes et al, Resp Care, 2020)
(Haynes et al, Resp Care, 2020)


Once you have diagnosed a patient with COPD, the next step is to assess it. You do this by asking about symptoms and exacerbation history.

I like to use the mMRC to ask about symptoms, because I can do it on the fly with no form.
“Do you have to stop for breath while walking around the grocery store?”
Yes bumps them up from low symptoms to high.
“Do you have to stop for breath while walking around the grocery store?”
Yes bumps them up from low symptoms to high.

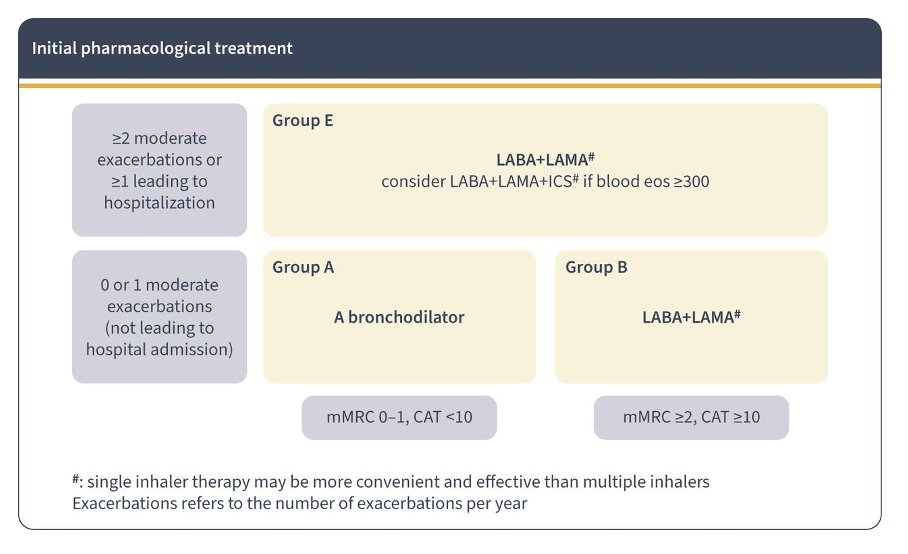
1 exacerbation that puts them in the hospital or 2 outpatient exacerbations/year puts them in the GOLD E (for exacerbation) category.

There are 3 main inhaled maintenance meds we use in COPD—LABA, LAMA, and ICS. The focus in most COPD is on bronchodilators (vs ICS in asthma).

There are approximately 1 million inhalers, and you don’t need to memorize them. You just need to know the classes and when to use them, and you can look up the rest.

GOLD makes it easy to know where to start with our handy dandy ABE GOLD groups.
GOLD A = any bronchodilator
GOLD B = LABA/LAMA combo
GOLD E = LABA/LAMA combo*
*ICS in some
GOLD A = any bronchodilator
GOLD B = LABA/LAMA combo
GOLD E = LABA/LAMA combo*
*ICS in some
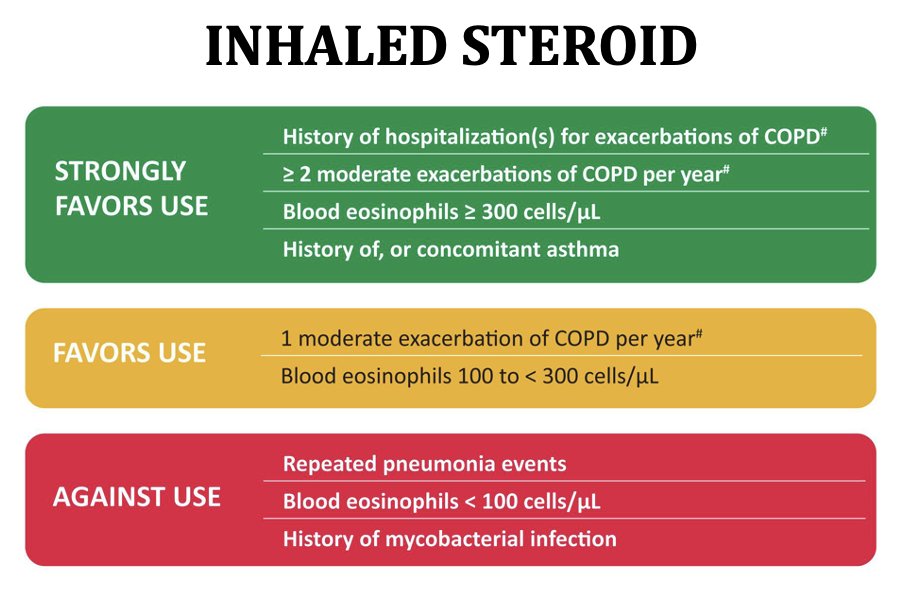
Notice that ICS is not first line for any group?
When to consider ICS: high eos, GOLD E, history of asthma.
ICS can increase risk of PNA and cause thrush, reducing adherence to inhalers. Have a reason you’re using it!
When to consider ICS: high eos, GOLD E, history of asthma.
ICS can increase risk of PNA and cause thrush, reducing adherence to inhalers. Have a reason you’re using it!
Other beneficial things to consider:
🔹Vaccinations – everyone!
🔹A1AT screening – everyone!
🔹Pulm rehab – GOLD B, E
🔹Lung CA screening – age 50-80, 20+ pack/years, current smoking or quit <15 years ago
🔹Roflumilast/azith – GOLD E
🔹Home O2 – resting hypoxia
🔹Vaccinations – everyone!
🔹A1AT screening – everyone!
🔹Pulm rehab – GOLD B, E
🔹Lung CA screening – age 50-80, 20+ pack/years, current smoking or quit <15 years ago
🔹Roflumilast/azith – GOLD E
🔹Home O2 – resting hypoxia
🔹NIV – stable COPD, marked daytime hypercapnia, no OSA
🔹Lung volume reduction
🔹Lung txp referral
🔹Lung volume reduction
🔹Lung txp referral
There's lots of interesting things happening in COPD--checkout the COPDGene study and SPIROMICS just as a start.
But the information here will give you a good foundation to help you take good care of your COPD patients (over 16 million people in the US)!
But the information here will give you a good foundation to help you take good care of your COPD patients (over 16 million people in the US)!
Ugh, I knew I would forget something.
Smoking cessation for everyone! Varenicline is first line, nicotine replacement is sometimes easier for patients (I like basal bolus approach, with patch + gum or lozenge for cravings).
Smoking cessation for everyone! Varenicline is first line, nicotine replacement is sometimes easier for patients (I like basal bolus approach, with patch + gum or lozenge for cravings).
https://twitter.com/MikeRoseMDMPH/status/1687287121046917120?s=20
• • •
Missing some Tweet in this thread? You can try to
force a refresh