1/Do you feel like you are drowning in an alphabet soup of stroke trials?
Want to ESCAPE the confusion about stroke treatment?
Let this #tweetorial DEFUSE the situation—w/an update on #stroke treatment from the July issue @TheAJNR
#medtwitter #meded #neurotwitter #FOAMed
Want to ESCAPE the confusion about stroke treatment?
Let this #tweetorial DEFUSE the situation—w/an update on #stroke treatment from the July issue @TheAJNR
#medtwitter #meded #neurotwitter #FOAMed

2/Stroke treatment began w/the discovery that the thrombolytic tPA could help improve outcomes in acute ischemic stroke.
tPA works on a clot in your artery like a drain cleaner does for a clog in your pipes—enzymatically breaking it down to relieve the obstruction
tPA works on a clot in your artery like a drain cleaner does for a clog in your pipes—enzymatically breaking it down to relieve the obstruction

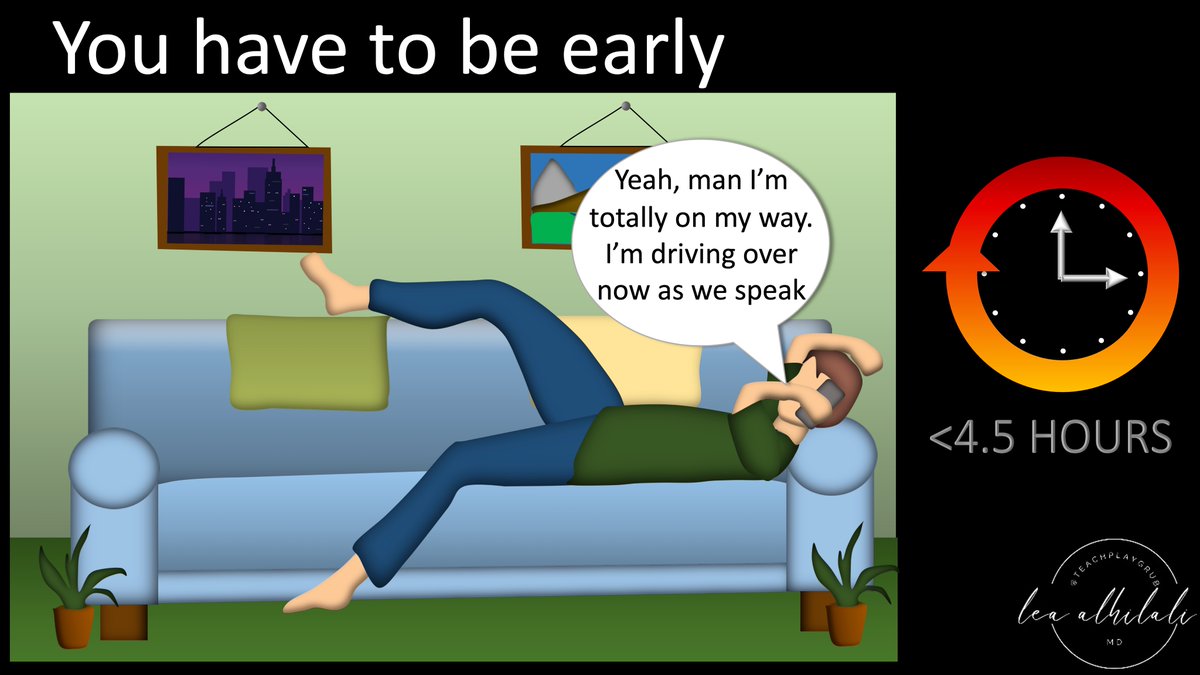
3/But there are big limitations to tPA.
First, it loses effectiveness quickly & can only be given early--w/in 4.5 hrs of last known normal (LKN).
Unfortunately, in real life, people are rarely early.
In fact, the vast majority of strokes occur after this time window
First, it loses effectiveness quickly & can only be given early--w/in 4.5 hrs of last known normal (LKN).
Unfortunately, in real life, people are rarely early.
In fact, the vast majority of strokes occur after this time window
4/Also it’s not very good for large vessel occlusions (LVO)
tPA is an enzyme, so it can only work on the exposed surface. Big clots have small surface area for their volume
Small surface area is the same reason a big ice cube takes waaay longer than expected to melt in a drink
tPA is an enzyme, so it can only work on the exposed surface. Big clots have small surface area for their volume
Small surface area is the same reason a big ice cube takes waaay longer than expected to melt in a drink

5/So when a drain cleaner doesn’t unclog the pipe, they go in & snake it out. Couldn’t we do the same w/large thrombus?
This is the principle behind thrombectomy—manually retrieving a clot that tPA is unlikely to dissolve.
Unfortunately, early studies failed to find benefit.
This is the principle behind thrombectomy—manually retrieving a clot that tPA is unlikely to dissolve.
Unfortunately, early studies failed to find benefit.

6/In 2013, 3 trials failed to show benefit of thrombectomy over tPA, complicating how endovascular therapy should be included in stroke treatment
However, the trials had many flaws—such as including patients w/no LVO. These were thrombectomy pts w/o a target for thrombectomy
However, the trials had many flaws—such as including patients w/no LVO. These were thrombectomy pts w/o a target for thrombectomy

7/It’s like if you aren’t very selective on a dating app. If you don’t look for people who are right for you—you might think there is no match for you.
Similarly, if you don’t select for patients who will benefit from thrombectomy, you might think thrombectomy doesn’t work
Similarly, if you don’t select for patients who will benefit from thrombectomy, you might think thrombectomy doesn’t work

8/The MR CLEAN trial changed all that w/new stent retrievers.
Stents had been used to try to open vessels & when they were pulled out, thrombus would come w/them. So they became thrombectomy devices.
You can remember MR CLEAN was when the vessel was finally CLEAN
Stents had been used to try to open vessels & when they were pulled out, thrombus would come w/them. So they became thrombectomy devices.
You can remember MR CLEAN was when the vessel was finally CLEAN

9/Testing the effectiveness of thrombectomy w/ old devices was like testing a cleaning device w/college students—hard to see if it makes a difference bc college kids never fully clean up anyways.
Stentrievers are like having your mom clean up—now you can see if it has an impact
Stentrievers are like having your mom clean up—now you can see if it has an impact

10/You can think of stroke treatment like apologies
Their effectiveness quickly wanes the longer you wait to give them—and if you wait too long, you are going to need more than just words
Similarly, the longer you wait, the more likely you will need something besides just tPA
Their effectiveness quickly wanes the longer you wait to give them—and if you wait too long, you are going to need more than just words
Similarly, the longer you wait, the more likely you will need something besides just tPA

11/Regardless of time, tPA may not be effective for large thrombus as previously mentioned.
It’s like if you made a BIG mistake—you may need more than words no matter how early you apologize.
It’s like if you made a BIG mistake—you may need more than words no matter how early you apologize.

12/LVOs are like making a BIG mistake. You can definitely apologize early, but that’s unlikely to resolve the issue.
Similarly, you can give tPA early for an LVO, but you’re going to need more.
LVOs need thrombectomy even w/tPA & tPA isn’t a contraindication to thrombectomy
Similarly, you can give tPA early for an LVO, but you’re going to need more.
LVOs need thrombectomy even w/tPA & tPA isn’t a contraindication to thrombectomy

13/But even the effectiveness of thrombectomy wanes w/time
It’s like cleaning up a stain—wait too long & the stain sets in—so no matter what cleaning agent you use, it’s impossible to get out.
Similarly, once the brain infarcts, even the most effective treatment can’t save it
It’s like cleaning up a stain—wait too long & the stain sets in—so no matter what cleaning agent you use, it’s impossible to get out.
Similarly, once the brain infarcts, even the most effective treatment can’t save it

14/So while the time from LKN matters, time until the brain infarcts matters more.
If we could select for those in whom brain hasn’t infarcted, treatment will be more effective—the stain hasn’t set in.
That is what the next generation of trials focused on—patient selection
If we could select for those in whom brain hasn’t infarcted, treatment will be more effective—the stain hasn’t set in.
That is what the next generation of trials focused on—patient selection

15/These trials looked for “mismatch”—ischemic brain that hasn’t yet fully infarcted
Like how Wall Street looks for under-valued stocks—stocks whose prices are too low w/potential for growth
Same w/thrombectomy—look for pts w/under-infarcted tissue w/potential for salvage
Like how Wall Street looks for under-valued stocks—stocks whose prices are too low w/potential for growth
Same w/thrombectomy—look for pts w/under-infarcted tissue w/potential for salvage

16/“Enough” tissue to salvage was:
--Mismatch ratio (between infarcted core & ischemic penumbra) on perfusion of 1.8
--Core infarct < 70cc (bc large infarcts were thought too devastating for salvage to help).
Remember this bc we save for retirement when we’re > 18 & < 70
--Mismatch ratio (between infarcted core & ischemic penumbra) on perfusion of 1.8
--Core infarct < 70cc (bc large infarcts were thought too devastating for salvage to help).
Remember this bc we save for retirement when we’re > 18 & < 70

17/Two trials proved that if correct patients were selected, endovascular therapy was effective even later than expected, DAWN & DEFUSE-3.
Remember this bc this was a new DAWN for stroke treatment & at dawn is when people like to have their essential oil DIFFUSER running.
Remember this bc this was a new DAWN for stroke treatment & at dawn is when people like to have their essential oil DIFFUSER running.

18/So if LKN is <4.5 hrs, pt can get tPA
If they are pt w/an LVO, they also need thrombectomy, regardless of tPA—& this can happen up to 6 hours
After 6 hours, those w/an LVO should get thrombectomy if their perfusion imaging shows they still have significant salvageable brain
If they are pt w/an LVO, they also need thrombectomy, regardless of tPA—& this can happen up to 6 hours
After 6 hours, those w/an LVO should get thrombectomy if their perfusion imaging shows they still have significant salvageable brain

19/It’s like a marathon. Early on, everyone’s still in—besides obvious contraindications, everyone can get tPA early
But as time passes, farther along on the course, less & less people are still in the running
Longer time from LKN, means it’s more selective & less are eligible
But as time passes, farther along on the course, less & less people are still in the running
Longer time from LKN, means it’s more selective & less are eligible

20/How do you remember the timing? Well, it’s like how you select people.
Before 4:30, it’s just meeting people for coffee. You’ll meet anyone, unless they have like a lizard tail
Same w/strokes, unless obvious contraindication (hemorrhage, etc), everyone can get tPA < 4.5 hrs
Before 4:30, it’s just meeting people for coffee. You’ll meet anyone, unless they have like a lizard tail
Same w/strokes, unless obvious contraindication (hemorrhage, etc), everyone can get tPA < 4.5 hrs

21/Now before 6:00pm, it’s happy hour. So you’re a little more selective about who buys you a drink.
You don’t want anyone puny & on a scale from 1 to 10, they’ve gotta be above average (>5).
Same w/strokes, before 6hrs, only BIG occlusions & ASPECTS >/= 6 get thrombectomy
You don’t want anyone puny & on a scale from 1 to 10, they’ve gotta be above average (>5).
Same w/strokes, before 6hrs, only BIG occlusions & ASPECTS >/= 6 get thrombectomy

22/Now after 6pm, it's into the night & things are a little more sketchy
You must be careful. Not only do you have the happy hour criteria—you must make sure they aren’t already committed to someone
Same w/stroke, after 6, must make sure they aren't already committed to infarct
You must be careful. Not only do you have the happy hour criteria—you must make sure they aren’t already committed to someone
Same w/stroke, after 6, must make sure they aren't already committed to infarct

23/So just think about how you would handle yourself:
At afternoon coffee (everyone welcome)
At happy hour (more selective for a bigger catch)
At the club (must make sure they aren’t already committed to going w/someone else)
At afternoon coffee (everyone welcome)
At happy hour (more selective for a bigger catch)
At the club (must make sure they aren’t already committed to going w/someone else)

24/But things are changing!
Studies have shown puny guys (distal & PCA occlusions) are worth a chance
Even guys who aren’t above 6 on a 1 to 10 scale (ASPECTS 3-5) can benefit
So just like trying to decide on a date, it comes down to the individual—the individual stroke pt
Studies have shown puny guys (distal & PCA occlusions) are worth a chance
Even guys who aren’t above 6 on a 1 to 10 scale (ASPECTS 3-5) can benefit
So just like trying to decide on a date, it comes down to the individual—the individual stroke pt

25/Hopefully, now this will be a new DAWN in your understanding of stroke treatment!
But this has just touched the surface. There's so much more—check out the full review at @AJNR. It's🆓 & #openaccess to all!
You’ll find it a stroke of genius!ajnr.org/content/44/7/7…
But this has just touched the surface. There's so much more—check out the full review at @AJNR. It's🆓 & #openaccess to all!
You’ll find it a stroke of genius!ajnr.org/content/44/7/7…
• • •
Missing some Tweet in this thread? You can try to
force a refresh