
Neuroradiologist @HRInstitute_AZ. @BarrowNeuro. Striving to make learning neuroimaging and anatomy fun. If I can make you laugh, I can make you learn.
 @TheAJNR 2/Everyone knows brain blood.
@TheAJNR 2/Everyone knows brain blood. 
 2/MRI & CT are like nuclear & coal power, respectively. Everyone knows CT is worse for you & usually MRI is very safe & better for your body
2/MRI & CT are like nuclear & coal power, respectively. Everyone knows CT is worse for you & usually MRI is very safe & better for your body
 2/First anatomy.
2/First anatomy.
 2/Strokes evolve, or grow old, the same way people evolve or grow old
2/Strokes evolve, or grow old, the same way people evolve or grow old
 2/The most common functional imaging used in dementia is FDG PET. And the most common dementia is Alzheimer’s disease (AD).
2/The most common functional imaging used in dementia is FDG PET. And the most common dementia is Alzheimer’s disease (AD). 
 2/Let’s start w/T1—it is #1 after all! T1 is for anatomy
2/Let’s start w/T1—it is #1 after all! T1 is for anatomy
 2/Temporal lobe can be divided centrally & peripherally.
2/Temporal lobe can be divided centrally & peripherally.
 2/The growing strength is for larger & larger field strengths for higher & higher resolution
2/The growing strength is for larger & larger field strengths for higher & higher resolution
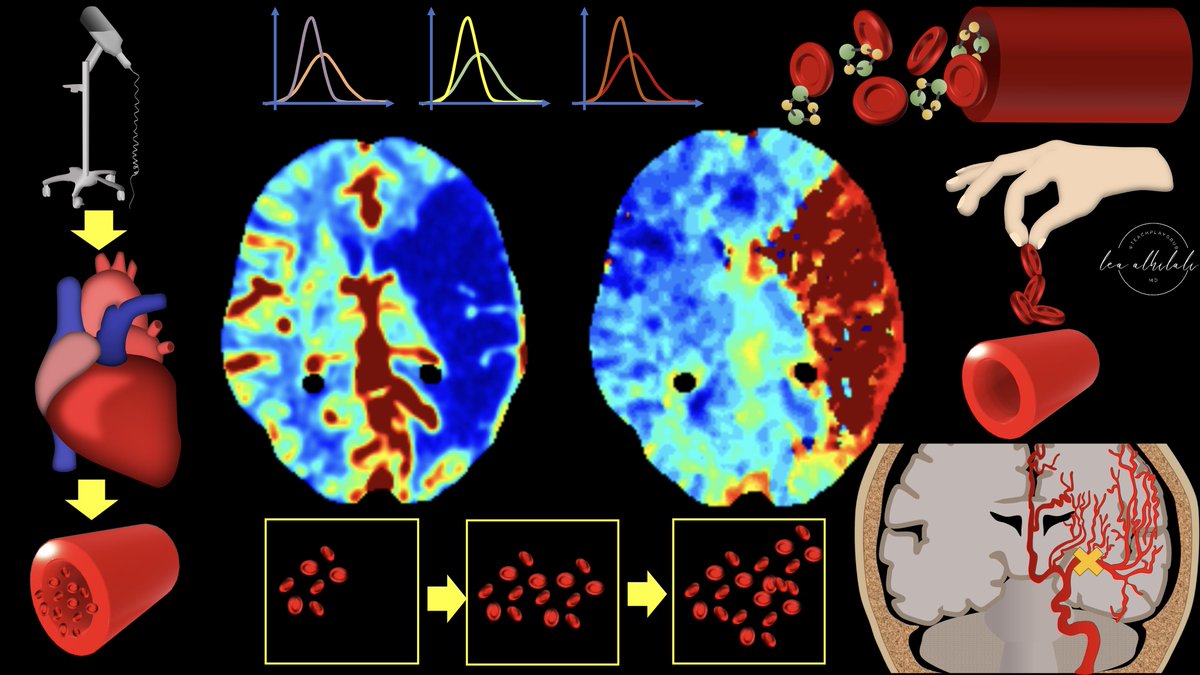
 @TheAJNR 2/Perfusion imaging is based on one principle: When you inject CT or MR intravenous contrast, the contrast flows w/blood & so contrast can be a surrogate marker for blood.
@TheAJNR 2/Perfusion imaging is based on one principle: When you inject CT or MR intravenous contrast, the contrast flows w/blood & so contrast can be a surrogate marker for blood.
 2/Anatomy of the inferior frontal gyrus (IFG) is best seen on the sagittal images, where it looks like the McDonald’s arches.
2/Anatomy of the inferior frontal gyrus (IFG) is best seen on the sagittal images, where it looks like the McDonald’s arches.
 2/Let’s start at the top. At the vertex is the superior frontal gyrus. This is easy to remember, bc it’s at the top—and being at the top is superior. It’s like the superior king at the top of the vertex.
2/Let’s start at the top. At the vertex is the superior frontal gyrus. This is easy to remember, bc it’s at the top—and being at the top is superior. It’s like the superior king at the top of the vertex. 
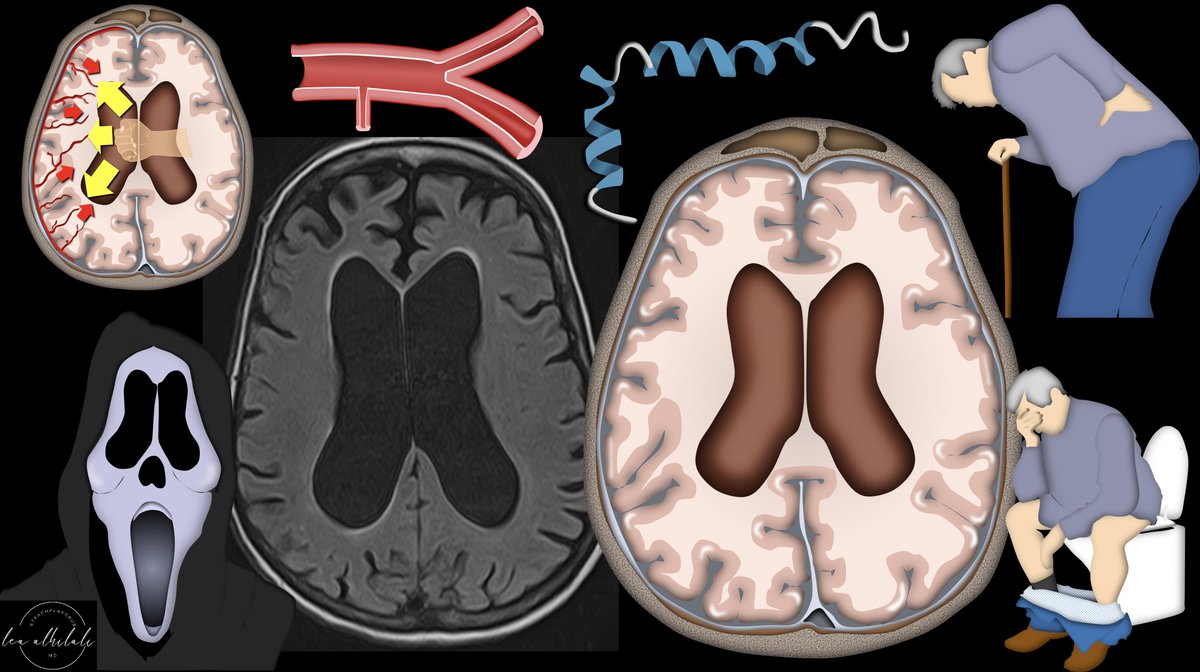 2/First, you must understand the pathophysiology of “idiopathic” or iNPH.
2/First, you must understand the pathophysiology of “idiopathic” or iNPH.
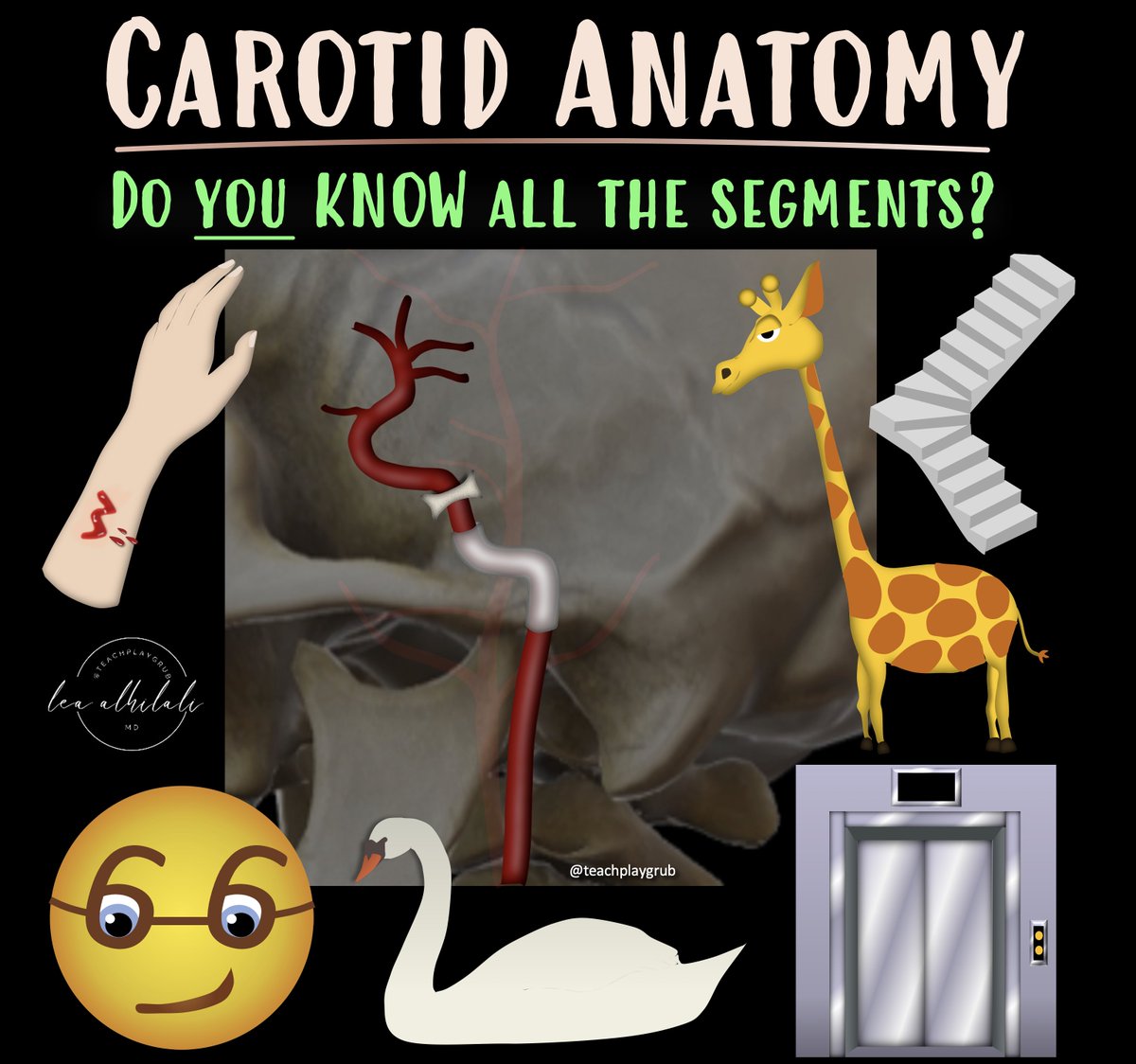 2/ICA is like a staircase—winding up through important anatomic regions like a staircase winding up to each floor Lobby is the neck.
2/ICA is like a staircase—winding up through important anatomic regions like a staircase winding up to each floor Lobby is the neck. 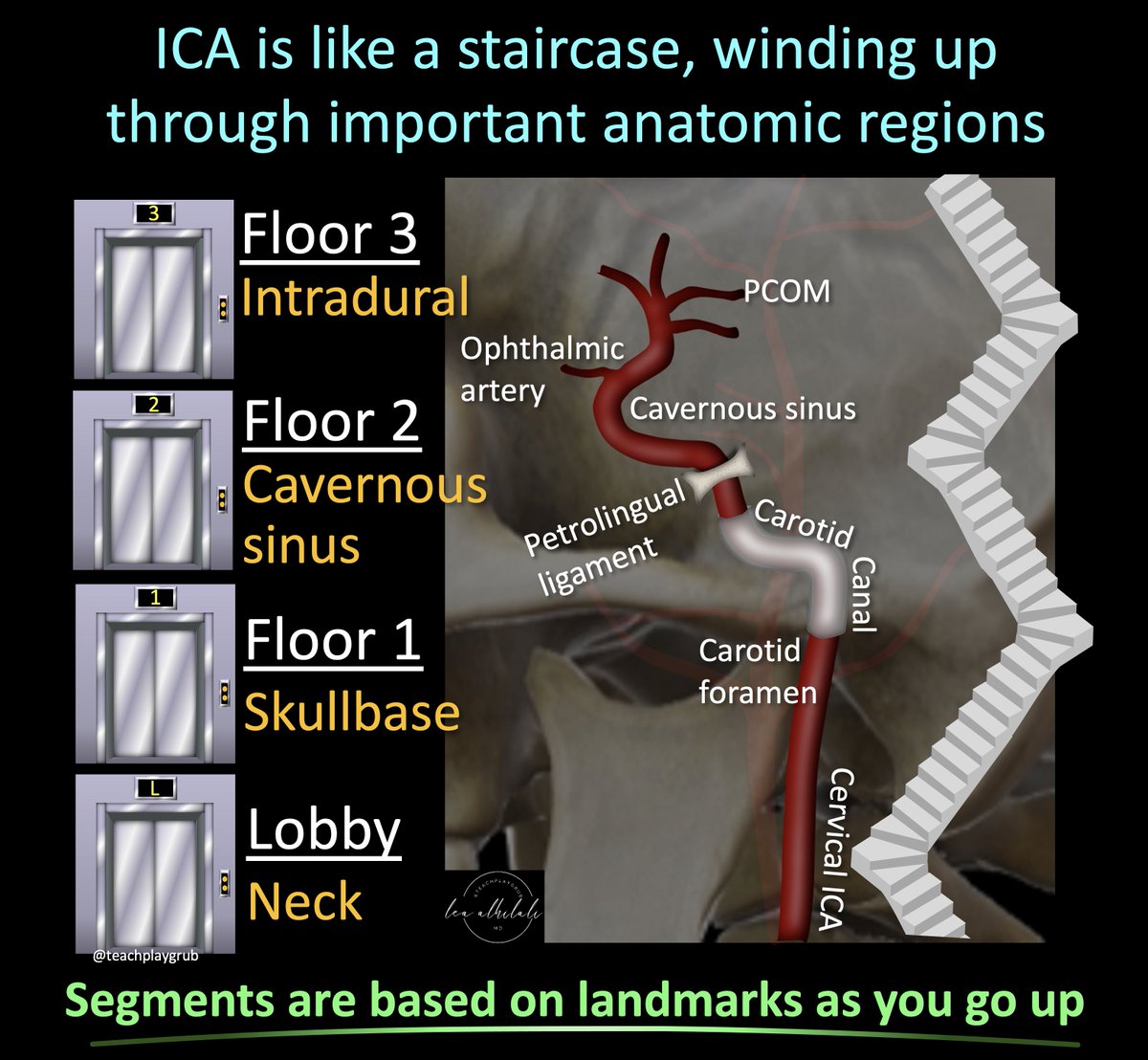
 2/Everyone knows the NASCET criteria:
2/Everyone knows the NASCET criteria: 
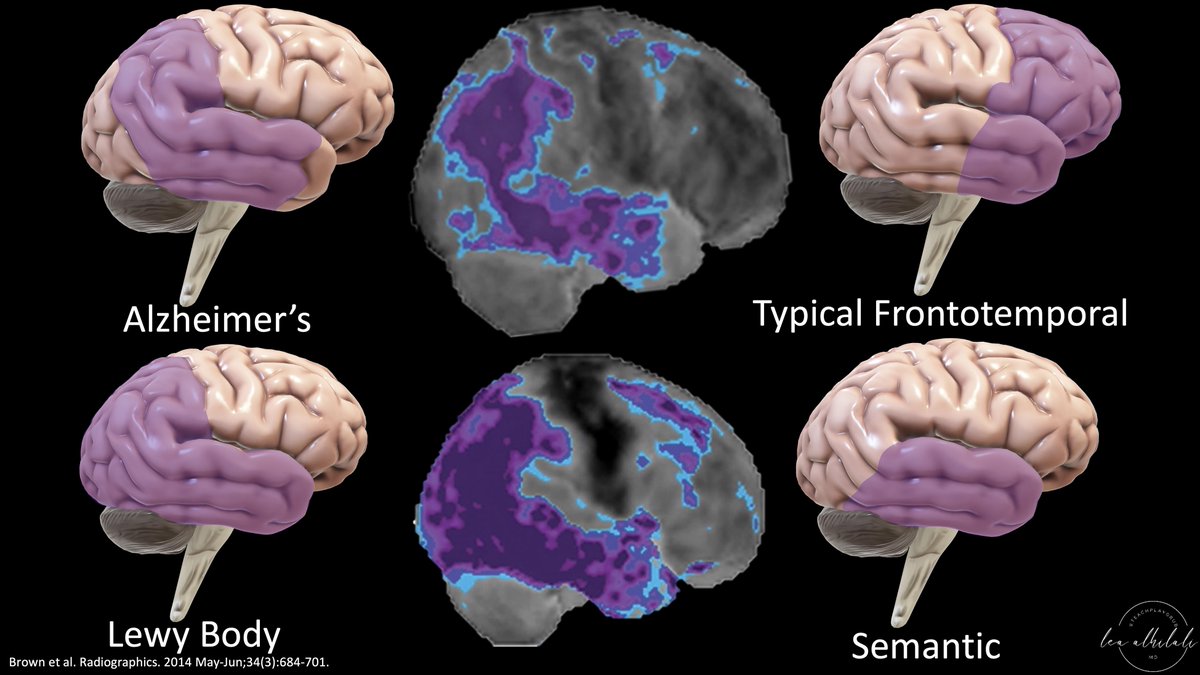 2/The most common functional imaging used in dementia is FDG PET. And the most common dementia is Alzheimer’s disease (AD).
2/The most common functional imaging used in dementia is FDG PET. And the most common dementia is Alzheimer’s disease (AD). 
 2/Perfusion imaging is based on one principle: When you inject CT or MR intravenous contrast, the contrast flows w/blood & so contrast can be a surrogate marker for blood.
2/Perfusion imaging is based on one principle: When you inject CT or MR intravenous contrast, the contrast flows w/blood & so contrast can be a surrogate marker for blood.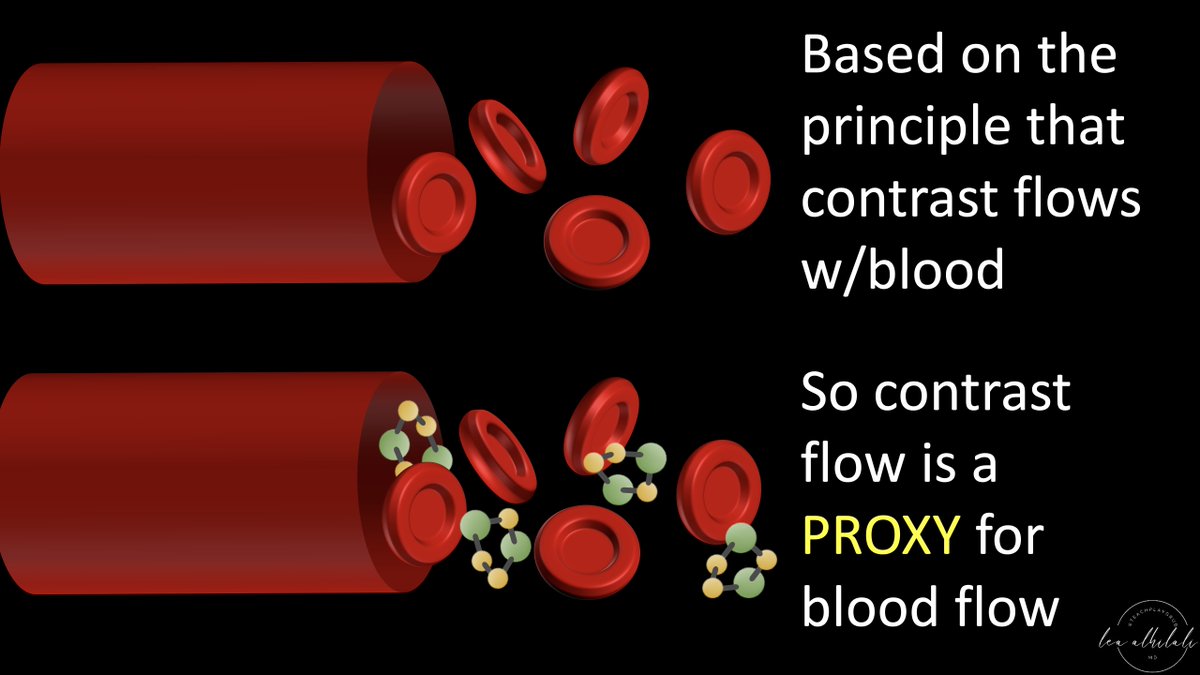
 2/Now the ninja turtle isn’t an actual sign—yet!
2/Now the ninja turtle isn’t an actual sign—yet!
 2/The first step is to insert the endoscope into the nasal cavity.
2/The first step is to insert the endoscope into the nasal cavity. 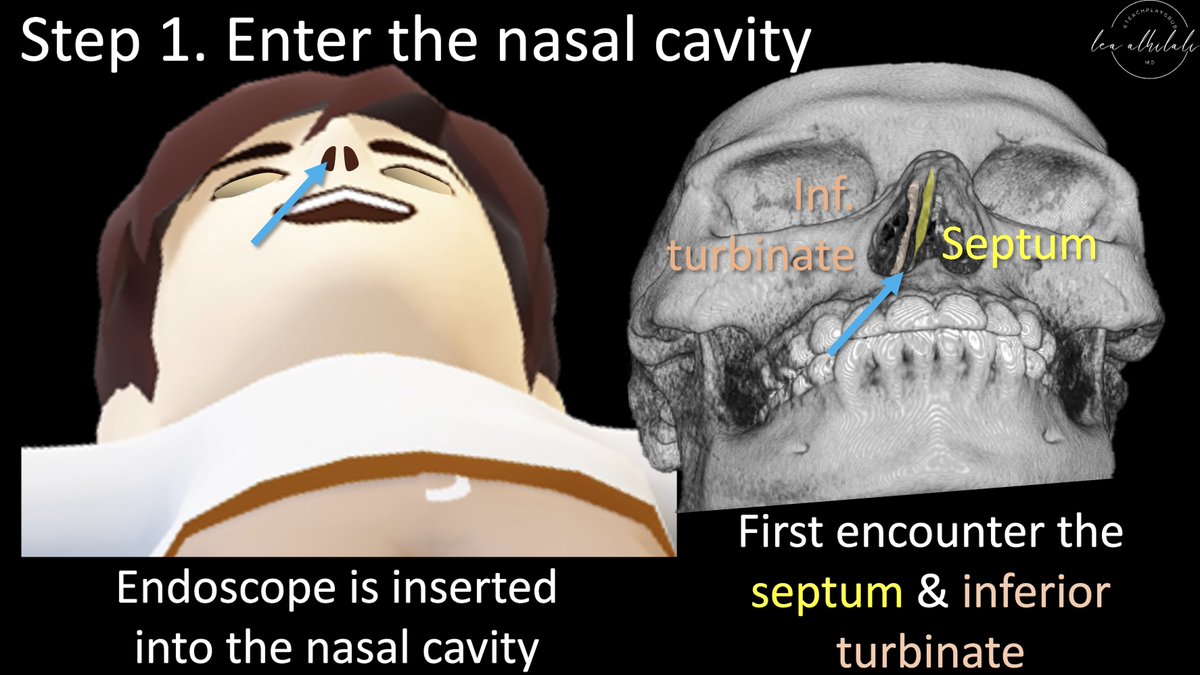
 2/First anatomy.
2/First anatomy.
 2/TLICS scores a fx on (1) morphology & (2) posterior ligamentous complex injury
2/TLICS scores a fx on (1) morphology & (2) posterior ligamentous complex injury
 2/The PPF is a crossroads between the skullbase & the extracranial head and neck
2/The PPF is a crossroads between the skullbase & the extracranial head and neck