Since ppl are talking about the "other" shot lately, I want make 3 points that build on seasonal data from Chicago (graph below).
1) There is no bigger racket than the flu shot.
▪️Changes every year
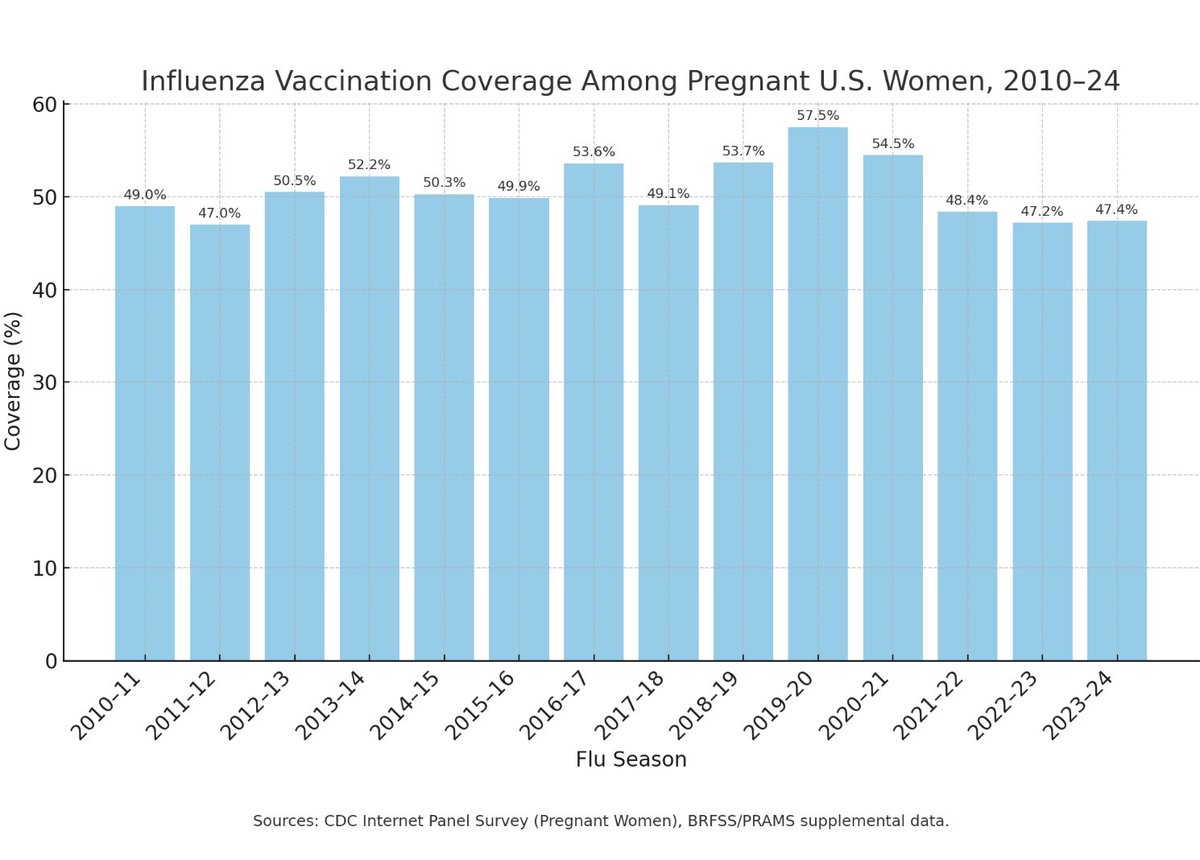
▪️Uptake fairly high (in the U.S.)
▪️Kids were roped in to the operation
▪️Widely acknowledged to not work well for the elderly (including by the CDC's flu expert)
▪️No one questions whether it has adverse effects, whether it causes/worsens respiratory illness, or can be deadly
▪️ People equate "not working" with "they guessed the wrong strain this year"
Sounds like a cash cow, right?
Imagine it wasn't simply "not working" but making things worse?
Imagine you need a new platform because all your messing around with the shot since 2009 is getting out of hand but you can only hide it for so long.
Imagine people aren't scared of flu but you've got those universal flu shot goals and all that investment in pandemic planning?
What would you do?
2) Many things that have been "done with" SARS-CoV-2/COVID were already being done with influenza, on a smaller scale. It wasn't new on the scene in 2020.
That includes but is not limited to
▪️PCR testing
▪️labeling ICU hospitalizations as flu associated based on a test result
▪️tracking vaccination status
▪️influenza-positive pneumonia deaths
The idea that these practices in the COVID Era are mistakes, brand new to the people asked to apply them, etc. is incorrect.
You don't "suddenly" foist these things on state/local public health agencies, healthcare workers, etc. You till the soil and leverage preexisting systems and practices.
3) The COVID shot/boosters/combo shots are not the only injections in the 2020-2023 mix. There has been widespread use of sedatives (for "calming" care home residents and people in ambulances, for putting people on vents) AND the flu shot.
Where's all cause mortality by flu shot status, I wonder?
Where's all mortality by flu shot & COVID shot status?
It seems people who do good work trying to tease out COVID shot problems are either forgetting or ignoring the flu shot, as though it doesn't matter.
In my opinion, starting the timeline in March 2020 or December 2020 is a mistake.
Limiting one's view to Virus From Wuhan and COVID shots is also a mistake.
Thank you for coming to my TED Talk.
1) There is no bigger racket than the flu shot.
▪️Changes every year
▪️Uptake fairly high (in the U.S.)
▪️Kids were roped in to the operation
▪️Widely acknowledged to not work well for the elderly (including by the CDC's flu expert)
▪️No one questions whether it has adverse effects, whether it causes/worsens respiratory illness, or can be deadly
▪️ People equate "not working" with "they guessed the wrong strain this year"
Sounds like a cash cow, right?
Imagine it wasn't simply "not working" but making things worse?
Imagine you need a new platform because all your messing around with the shot since 2009 is getting out of hand but you can only hide it for so long.
Imagine people aren't scared of flu but you've got those universal flu shot goals and all that investment in pandemic planning?
What would you do?
2) Many things that have been "done with" SARS-CoV-2/COVID were already being done with influenza, on a smaller scale. It wasn't new on the scene in 2020.
That includes but is not limited to
▪️PCR testing
▪️labeling ICU hospitalizations as flu associated based on a test result
▪️tracking vaccination status
▪️influenza-positive pneumonia deaths
The idea that these practices in the COVID Era are mistakes, brand new to the people asked to apply them, etc. is incorrect.
You don't "suddenly" foist these things on state/local public health agencies, healthcare workers, etc. You till the soil and leverage preexisting systems and practices.
3) The COVID shot/boosters/combo shots are not the only injections in the 2020-2023 mix. There has been widespread use of sedatives (for "calming" care home residents and people in ambulances, for putting people on vents) AND the flu shot.
Where's all cause mortality by flu shot status, I wonder?
Where's all mortality by flu shot & COVID shot status?
It seems people who do good work trying to tease out COVID shot problems are either forgetting or ignoring the flu shot, as though it doesn't matter.
In my opinion, starting the timeline in March 2020 or December 2020 is a mistake.
Limiting one's view to Virus From Wuhan and COVID shots is also a mistake.
Thank you for coming to my TED Talk.

Will get back to my flu series soon, but here are the first posts.
Human Interference, NOT Viral Interference
woodhouse76.com/p/flu-disppear…
Human Interference, NOT Viral Interference
woodhouse76.com/p/flu-disppear…
Data for the 2017-2018 season in Chicago (a "bad flu season")
▪️582 liberally-defined Flu-Associated ICU Hospitalizations
▪️10% of Flu-Associated ICU Hospitalizations Died
▪️Shot Status known for 60% of Flu-Associated ICU Hospitalizations
▪️50% of Flu-Associated ICU Hospitalizations with Known Shot Status Received the Flu Shot
▪️Flu shot status of Flu-associated deaths not given
▪️ No way of knowing flu shot status of the 40% for whom flu shot status wasn't reported
This should sound familiar.
I am NOT saying SARS-CoV-2 "is" influenza.
I'm saying the testing and data and counting/reporting frameworks are very similar to what had already been occurring with flu.
That's a big reason we did not see people who work inside hospitals, care homes, and health agencies doubt what they were being told to do.
▪️582 liberally-defined Flu-Associated ICU Hospitalizations
▪️10% of Flu-Associated ICU Hospitalizations Died
▪️Shot Status known for 60% of Flu-Associated ICU Hospitalizations
▪️50% of Flu-Associated ICU Hospitalizations with Known Shot Status Received the Flu Shot
▪️Flu shot status of Flu-associated deaths not given
▪️ No way of knowing flu shot status of the 40% for whom flu shot status wasn't reported
This should sound familiar.
I am NOT saying SARS-CoV-2 "is" influenza.
I'm saying the testing and data and counting/reporting frameworks are very similar to what had already been occurring with flu.
That's a big reason we did not see people who work inside hospitals, care homes, and health agencies doubt what they were being told to do.

This is from the last surveillance report of that same season. chicago.gov/city/en/depts/…
Not sure why the death number is lower here than in the data file.
Note that ventilator support for ICU hospitalizations is report. No data for how many of the deaths were on ventilators.
Death definition is "Date of death occurring within one week of positive influenza test."
Again, this should all sound familiar
Not sure why the death number is lower here than in the data file.
Note that ventilator support for ICU hospitalizations is report. No data for how many of the deaths were on ventilators.
Death definition is "Date of death occurring within one week of positive influenza test."
Again, this should all sound familiar

Interesting that positive flu tests "disappeared" for the 2020-21 season, but the reporting of adverse effects from the flu shot did not.
https://x.com/DrGooglybean/status/1710750478143827998?s=20
Case in point.
This was going on before 2020.
This was going on before 2020.
https://twitter.com/coachmarcsmith/status/1710753131301155209
This illustrates part of what I’m saying.
How would this ever be disentangled in the COVID shot studies, or in any study of mortality?
It’s chaos.
(Which is probably the point)
How would this ever be disentangled in the COVID shot studies, or in any study of mortality?
It’s chaos.
(Which is probably the point)
https://twitter.com/AlexClark114/status/1710788252708335875
Also proves my point
Historically, “Flu shot failed this year” or “I got the flu shot but got flu anyway” hasn’t really done much to assail the flu shot’s uptake appreciably
Don’t people wonder how “bad” flu season would end up being if uptake were 5-10%?
I do.
Historically, “Flu shot failed this year” or “I got the flu shot but got flu anyway” hasn’t really done much to assail the flu shot’s uptake appreciably
Don’t people wonder how “bad” flu season would end up being if uptake were 5-10%?
I do.
https://twitter.com/TheLegalBrain1/status/1711023544191025619
To those who think the govt’s claims about the COVID shot are unique or something new under the sun, sorry to say, that is NOT the case.
Peter Doshi is undefeated on this topic. 🔥🔥🔥
BMJ, 2013 ⬇️
“Promotion of influenza vaccines is one of the most visible and aggressive public health policies today. Twenty years ago, in 1990, 32 million doses of influenza vaccine were available in the United States. Today around 135 million doses of influenza vaccine annually enter the US market, with vaccinations administered in drug stores, supermarkets—even some drive-throughs. This enormous growth has not been fueled by popular demand but instead by a public health campaign that delivers a straightforward, who-in-their-right-mind-could-possibly-disagree message: influenza is a serious disease, we are all at risk of complications from influenza, the flu shot is virtually risk free, and vaccination saves lives. Through this lens, the lack of influenza vaccine availability for all 315 million US citizens seems to border on the unethical. Yet across the country, mandatory influenza vaccination policies have cropped up, particularly in healthcare facilities,1 precisely because not everyone wants the vaccination, and compulsion appears the only way to achieve high vaccination rates. Closer examination of influenza vaccine policies shows that although proponents employ the rhetoric of science, the studies underlying the policy are often of low quality, and do not substantiate officials’ claims. The vaccine might be less beneficial and less safe than has been claimed, and the threat of influenza appears overstated.” bmj.com/content/346/bm…
Peter Doshi is undefeated on this topic. 🔥🔥🔥
BMJ, 2013 ⬇️
“Promotion of influenza vaccines is one of the most visible and aggressive public health policies today. Twenty years ago, in 1990, 32 million doses of influenza vaccine were available in the United States. Today around 135 million doses of influenza vaccine annually enter the US market, with vaccinations administered in drug stores, supermarkets—even some drive-throughs. This enormous growth has not been fueled by popular demand but instead by a public health campaign that delivers a straightforward, who-in-their-right-mind-could-possibly-disagree message: influenza is a serious disease, we are all at risk of complications from influenza, the flu shot is virtually risk free, and vaccination saves lives. Through this lens, the lack of influenza vaccine availability for all 315 million US citizens seems to border on the unethical. Yet across the country, mandatory influenza vaccination policies have cropped up, particularly in healthcare facilities,1 precisely because not everyone wants the vaccination, and compulsion appears the only way to achieve high vaccination rates. Closer examination of influenza vaccine policies shows that although proponents employ the rhetoric of science, the studies underlying the policy are often of low quality, and do not substantiate officials’ claims. The vaccine might be less beneficial and less safe than has been claimed, and the threat of influenza appears overstated.” bmj.com/content/346/bm…
Imagine how many adverse events from flu shot were unreported as such due to
a) Doctor/nurse/patient resistance to seeing them as such
b) patients thinking of adverse events involving flu-like illness as “getting flu anyway”
The COVID racket is the flu racket on steroids.
a) Doctor/nurse/patient resistance to seeing them as such
b) patients thinking of adverse events involving flu-like illness as “getting flu anyway”
The COVID racket is the flu racket on steroids.
Great example of how doctors are conditioned to think certain ways about drugs, shots, etc.
https://twitter.com/sukicat2568/status/1711190083267592493
I am NOT saying the pathogen identified as SARS-CoV-2 is an influenza virus.
I AM saying the things we’ve seen with “COVID” were already being done with ILI/influenza.
The goal has long been “One Shot to Rule Them All”
Them = so-called seasonal respiratory pathogens
I AM saying the things we’ve seen with “COVID” were already being done with ILI/influenza.
The goal has long been “One Shot to Rule Them All”
Them = so-called seasonal respiratory pathogens
I also not suggesting influenza and The Flu Shot/Flu Surveillance Regime were the WHY of the COVID operation.
I'm saying it laid the groundwork significant portions of the HOW.
I'm saying it laid the groundwork significant portions of the HOW.
So, did anyone have concerns about ppl receiving
a flu shot in Sept 2020,
a COVID shot in Dec 2020/Jan 2021,
then a flu shot in Sept 2021,
then a COVID booster in Nov 2021,
followed by a COVID booster in April 2021,
& another flu shot in Sept 2022...
a flu shot in Sept 2020,
a COVID shot in Dec 2020/Jan 2021,
then a flu shot in Sept 2021,
then a COVID booster in Nov 2021,
followed by a COVID booster in April 2021,
& another flu shot in Sept 2022...
https://x.com/the_rostrich/status/1711190130424479774?s=20
Another 🧵 from me, explaining that I am NOT saying SARS-CoV-2 is rebranded flu.
I also take issue w/ “all COVID deaths are pneumonia deaths.”
That’s an errant, if well-meaning, claim made by people who do not quite understand the basics of & limitations around coding deaths
I also take issue w/ “all COVID deaths are pneumonia deaths.”
That’s an errant, if well-meaning, claim made by people who do not quite understand the basics of & limitations around coding deaths
https://twitter.com/Wood_House76/status/1706648190290694227
Not quite.
What people don’t realize is that the flu surveillance program WAS increasingly being used to attribute more pneumonia & influenza deaths to influenza — w/out compromising the flu shot reputation as an jab that maybe didn’t work great but wasn’t seen as harmful
What people don’t realize is that the flu surveillance program WAS increasingly being used to attribute more pneumonia & influenza deaths to influenza — w/out compromising the flu shot reputation as an jab that maybe didn’t work great but wasn’t seen as harmful
https://twitter.com/StillShakinIt/status/1706650781263237445
The number of SARS-CoV-2 tests given in three months in NYC was more than DOUBLE the number of flu tests given the entire season.
What exactly were these tests picking up?
What exactly were these tests picking up?
https://x.com/Wood_House76/status/1711413957867581464?s=20
Tangent: King County, WA (Gate-Funded Seattle Project Territory) weekly flu tests given vs Chicago, 2015-2022
What do we make of this?
I see earnest efforts of some kind. 🧐
Also, fewer flu tests given in both cities in 2020-21 season.
What do we make of this?
I see earnest efforts of some kind. 🧐
Also, fewer flu tests given in both cities in 2020-21 season.

Gates*
As in Bill :)
As in Bill :)
Operation COVID was a resounding success
✅ One Shot to Rule Them All still on track
✅ “Pandemic Potential Pathogens”/“Global Health Threats” narratives still intact
✅ Old flu shot/surveillance program emerges unscathed
✅ One Shot to Rule Them All still on track
✅ “Pandemic Potential Pathogens”/“Global Health Threats” narratives still intact
✅ Old flu shot/surveillance program emerges unscathed
https://twitter.com/jengleruk/status/1717560644965138865
Another post with my questions/thoughts on the Flu Shot & Operation COVID
https://x.com/Wood_House76/status/1720878406911308068?s=20
@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh